Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Wilbert Huang
RSUD Natuna, Natuna, Kepulauan Riau, Indonesia.
Email: wilberthuang67@gmail.com
Received: Mar 27, 2026 Accepted: Apr 10, 2026 Published: Apr 17, 2026
Citation: Huang W, Charlex HJM, Farsal RA, Amadea MID, Hendrianus T. Catastrophic hemorrhagic complication post fibrinolysis in STEMI patient: A rare case report in a limited resource setting. Ann Case Rep Med Images. 2026; 3(1): 1083.
Copyright: Huang W et al. © All rights are reserved
Background: Despite the efficacy of fibrinolysis, it also imposes patient to risk of bleeding that could be fatal.
Case description: A 68-year-old male presented with anginal chest pain 4 hours onset. Vital signs were BP 59/40 mmHg, HR 45×/minute, RR 22×/minute and SpO2 88%. Patient had history of PCI on 2015. Electrocardiogram showed ST-elevation in lead II, III, and aVF and ST-depression in all precordial leads suggesting inferior STEMI. Laboratory findings showed leukocytosis, elevated liver and CK-MB markers and eGFR 49. Chest radiography revealed fibrotic infiltration in upper left thorax, suggesting tuberculosis infection. Successful and uneventful fibrinolysis with streptokinase was done with ST-segment resolution. Patient was additionally given fondaparinux, bisoprolol, and atorvastatin. Four hours post-fibrinolysis, patient developed right facial drooping and extremities weakness, and slurred speech, suggestive of a stroke and CT-scan showed acute lacunar infarct in left pons. Seven hours post-fibrinolysis, patient experienced respiratory distress with SpO2 dropping to 83% and was indicated for intubation. During preoxygenation, patient developed massive hemoptysis and hematemesis suggesting gastrointestinal and alveolar bleeding. Patient’s estimated blood loss was 2000 ml. Patient was administered tranexamic acid, vitamin K, and high dose PPI. Patient was planned for PRC blood transfusion but unfortunately, patient developed ventricular tachycardia and did not survive.
Discussion: Currently, no validated bleeding risk score exists to assess STEMI patient undergoing fibrinolytic therapy. Hence, individualized bleeding risk stratification should be the priority.
Conclusion: Fibrinolysis can be both life-saving and life-threatening because of its potential to cause severe bleeding.
Keywords: Fibrinolysis; Bleeding; Alveolar hemorrhage; Acute coronary syndrome.
Fibrinolysis is an important pharmaco-invasive therapy for acute coronary syndrome patient particularly those with ST-segment elevation myocardial infarction that presented within 12 hours of symptoms onset and in condition when primary Percutaneous Coronary Intervention (PCI) cannot be achieved within 120 minutes. Current guideline recommends that despite successful or unsuccessful fibrinolytic, patient should still be referred for angiography and rescue PCI and readmission of fibrinolytic is no longer recommended in event of failed fibrinolysis [1].
However, despite its efficacy, fibrinolysis also imposes patient with bleeding risk that could occur either as mild to severe bleeding in various locations starting from vascular access sites and to internal hemorrhage in gastrointestinal, retroperitoneal, genitourinary, and cerebral systems [2]. One of the rare complications of fibrinolysis is pulmonary alveolar hemorrhage that could be catastrophic and fatal. Currently, there is no recommended bleeding risk score to stratify bleeding risk in STEMI patients undergoing fibrinolysis; therefore, individualized clinical judgment based on patient characteristics and comorbidities is required.
A 68-year-old male presented to the emergency department with typical anginal chest pain with 4 hours onset. The patient felt tightness in the chest that did not radiate to other body regions that did not resolve with resting. The patient had history of Percutaneous Coronary Intervention (PCI) on 2015 but the details of the intervention was not retrieved nor recalled by the patient. The patient claimed to be compliant on his medications and routinely controlled his condition with a cardiologist. The patient had history of hypertension and dyslipidemia that were well- controlled with medications.
Initially, the patient presented with vital signs of BP 59/40 mmHg, HR 45x/minute, RR 22x/minute and SpO2 88%. However, despite hypotensive with oxygen desaturation, the patient was clinically stable and was still able to communicate well and was not dyspnoeic. The patient also had no symptoms suggestive of pulmonary disease, such as coughing. Physical examinations revealed an adequate peripheral perfusion with less than 2 seconds of capillary refill time, strong peripheral pulse, and warm extremities. Auscultation of the lung fields also did not reveal any crackles/ rales nor were there any abnormalities in the heart sounds.
Electrocardiogram (ECG) was done in the patient within 10 minutes of presentation and the ECG result showed ST-elevation in lead II, III, and aVF and ST-depression in all precordial leads suggesting inferior ST segment elevation myocardial infarction (Figure 1). However, right sided (V3R and V4R) and posterior (V7–V9) leads were not examined. Laboratory findings showed leukocytosis, elevated liver and CK-MB markers (46.3 U/L) and eGFR 49 (Table 1). Additionally, chest radiography was also examined and revealed fibrotic infiltration in upper left thorax, suggesting tuberculosis infection (Figure 2). The working diagnosis at the moment was inferior STEMI with suspect tuberculosis infection. The patient was initially loaded with 325 mg of aspirin and 400 mg of clopidogrel. Patient was also started on dobutamine and norepinephrine titrated to reach mean arterial pressure >65 mmHg. The patient was also oxygenated to correct for the desaturation.
| Laboratory parameters | Value | Unit |
|---|---|---|
| Hemoglobin | 15.6 | g/ dL |
| Hematocrit | 46.9 | % |
| Leukocyte | 17.73 | 103/ ul |
| Thrombocyte | 165 | 103/ ul |
| Basophil | 0.1 | % |
| Eosinophil | 0 | % |
| Monocyte | 4.6 | % |
| Lymphocyte | 9.6 | % |
| Neutrophil | 85.7 | % |
| SGOT | 73 | u/L |
| SGPT | 61 | u/L |
| Ureum | 37 | mg/ dL |
| Creatinine | 1.53 | mg/ dL |
| CK- MB | 46.3 | U/L |
| Natrium | 144 | mmol/ L |
| Kalium | 3.6 | mmol/ L |
| Chloride | 106 | mmol/ L |
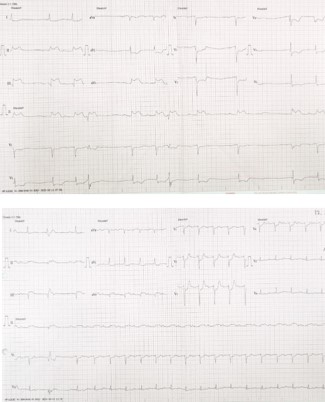
Figure 1: ECG findings showing ST segment elevation in inferior leads (above) and post fibrinolytic ST segment resolution (below).

Figure 2: Chest X ray of the patient revealing fibrotic infiltration in the upper left thorax.
Due to the limited-resource setting and the unavailability of a PCI center, the patient was treated with fibrinolysis using streptokinase at a dose of 1.5 million units. A careful and comprehensive assessment of the patient’s absolute and relative contraindications to fibrinolysis was performed, and none were identified. Fibrinolysis was successful with >50% ST segment elevation resolution (Figure 1) and was uneventful with no signs and symptoms of bleeding in any organ system. Patient was additionally given fondaparinux 2.5 mg subcutaneously, bisoprolol 1.25 mg, and atorvastatin 40 mg.
However, four hours post-fibrinolysis, patient suddenly developed right facial drooping with right extremities weakness, and slurred speech in the emergency department. The condition was highly suggestive of a stroke, initially suspected to be hemorrhagic of origin as a complication of fibrinolysis and anticoagulant use. The patient was then rushed for head CT scan to confirm the bleeding. However, CT-scan showed acute lacunar infarct in the left pons (Figure 3). The patient was then consulted to the neurology department and was advised to administer mannitol 4×125 ml when systolic blood pressure reaches above 110 mmHg. The patient was then transported to the Intensive Care Unit (ICU) for further observation.

Figure 3: Head CT scan of the patient revealing lacunar infarct in left pons.
Seven hours post-fibrinolysis, patient suddenly experienced shortness of breath with respiratory distress and oxygen saturation dropping to 83% from 95% on 12 Liters of oxygen on non- rebreather mask. The patient was then indicated for intubation. During preoxygenation with bag valve mask, patient developed massive hemoptysis and hematemesis suggesting gastrointestinal and alveolar bleeding. The estimated blood loss during the moment was 2000 ml and patient’s hemoglobin dropped from 15.6 to 13.4 g/dL. Emergency chest radiography was done and revealed alveolar pulmonary edema (Figure 4). With the massive bleeding, patient was administered tranexamic acid, vitamin K, and high dose PPI. Patient was also planned for pack red cell blood transfusion but unfortunately, after 2 hours of monitoring, patient developed ventricular tachycardia and the patient did not survive.
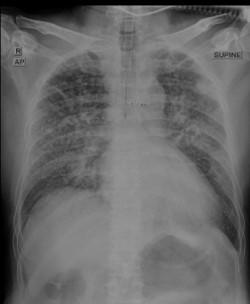
Figure 4: Chest X-ray of the patient revealing alveolar pulmonary edema following fibrinolysis, after the onset of hemoptysis.
Fibrinolysis remains an important and recommended pharmaco-invasive strategy for the management of ST-Segment Elevation Myocardial Infarction (STEMI) in selected patients. Prior to fibrinolytic therapy, careful history taking to identify relative and absolute contraindications is routinely performed to minimize the risk of major bleeding complications. Nevertheless, serious hemorrhagic events may still occur despite the absence of recognized contraindications, underscoring the need for an individualized assessment of bleeding risk in every patient.
In this report, we describe a rare and fatal case of pulmonary alveolar and gastrointestinal hemorrhage following fibrinolytic therapy in a patient with no relative or absolute contraindications. Pulmonary alveolar hemorrhage is an uncommon but potentially lethal complication of fibrinolysis, typically occurring within hours to days after administration. Clinical presentation often includes hemoptysis, acute anemia, and radiographic pulmonary infiltrates, with severity ranging from mild respiratory compromise to fulminant respiratory failure. Several pathophysiological mechanisms have been proposed, including underlying pulmonary parenchymal abnormalities, immune-mediated capillaritis (particularly associated with streptokinase), and prior defibrillation-related lung injury [3-5].
In our case, chest radiography revealed fibrotic infiltration in the left upper lung field, which may have predisposed the patient to pulmonary alveolar hemorrhage following fibrinolysis due to the inflamed lung parenchyma. Currently, no validated bleeding risk score exists specifically for patients with acute coronary syndrome undergoing fibrinolytic therapy, making risk stratification particularly challenging in this population. Certain patient characteristics in this case—such as advanced age, abnormal renal function, and elevated liver enzymes—may have suggested an increased bleeding risk, as these factors are incorporated into commonly used bleeding risk scores like HAS-BLED [6] and CRUSADE [7]. However, their applicability to fibrinolysis remains limited. Therefore, this case highlights the urgent need for the development of a validated bleeding risk assessment tool tailored to fibrinolytic therapy, to better balance ischemic benefit against bleeding risk in STEMI patients.
Fibrinolysis can be both life-saving and life-threatening because of its potential to cause severe bleeding. Therefore, individualized bleeding risk assessment before fibrinolysis is crucial to prevent fatal complications.