Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Mary Solou
Second Department of Neurosurgery, Attikon University General Hospital, National and Kapodistrian University of Athens Medical School, Athens, Greece.
Email: marysolou06@gmail.com
Received: Mar 20, 2026 Accepted: Apr 08, 2026 Published: Apr 15, 2026
Citation: Banos S, Solou M, Papadopoulos EK, Ydreos I, Stavrinou LC, et al. A rare case of giant pituitary metastasis from a duodenopancreatic neuroendocrine tumor and literature review. Ann Case Rep Med Images. 2026; 3(1): 1082.
Copyright: Solou M et al. © All rights are reserved
Background: Pituitary metastases are rare and often mimic benign adenomas, leading to diagnostic delays. Even more uncommon are metastases from gastrointestinal or pancreatic Neuroendocrine Tumors (NETs), especially when presenting as giant sellar masses.
Case presentation: We report a rare case of a giant pituitary metastasis from a duodenopancreatic NET. The patient, a 57-year-old male, presented with sudden neurological deterioration. Imaging revealed a giant sellar mass with suprasellar and intraventricular extension causing obstructive hydrocephalus. Emergency surgical decompression was performed. Histopathological analysis demonstrated a grade 2 Neuroendocrine Tumor (NET) consistent with a duodenopancreatic origin. Despite intervention, the patient developed postoperative complications and died. A focused literature review identified 23 reported cases of pituitary metastases from gastrointestinal or pancreatic NETs, most presenting with visual impairment, hypopituitarism, and invasive radiological features mimicking adenomas.
Conclusion: Pituitary metastasis from duodenopancreatic NETs is extremely rare but should be considered in rapidly progressive or atypical sellar lesions. Histological confirmation is essential for accurate diagnosis. Although surgical intervention offers symptom relief, the overall prognosis remains poor due to systemic disease progression.
Keywords: Pituitary metastasis; Neuroendocrine tumor; Pancreatic NET; Giant pituitary tumor; Sellar mass; Hypopituitarism.
Pituitary metastases are rare, accounting for approximately 1-3.6% of all surgically treated sellar lesions, but are increasingly recognized due to improved survival in cancer patients and advancements in imaging techniques and surveillance cancer pathways [1,2]. Their diagnosis poses significant challenges due to their radiological similarity to primary pituitary adenomas and often a non-specific clinical presentation [3]. Although breast and lung origin metastases are the most common in the pituitary gland, metastases from gastrointestinal and neuroendocrine tumors—including pancreas, thyroid, and colon—have also been documented, albeit far less frequently [3-9].
In the majority of cases, pituitary metastases remain clinically silent and thus undiagnosed. Literature has shown pituitary involvement in up to 28% of cancer patient autopsies, though the symptomatic cases remain infrequent [3,10]. In addition, metastatic Neuroendocrine Tumors (NETs) to the pituitary are even rarer but clinically significant contributors, occasionally presenting as “collision tumors” within pre-existing pituitary adenomas, often diagnosed intraoperatively or on histology [9,11,12]. Importantly, up to 44% of pituitary metastases are the initial manifestation of a previously undiagnosed malignancy, underscoring the need for high clinical suspicion [5].
While pituitary metastases are a challenge, as described, their combination with a giant pituitary lesion can complicate management. Giant pituitary adenomas constitute 6-15% of all pituitary lesions and pose substantial surgical and endocrinological challenges due to their size, invasiveness, and proximity to critical neurovascular structures [13,14]. These tumors often result in mass effect symptoms—visual impairment, headaches, cranial nerve palsies—as well as hypopituitarism, particularly when extending suprasellarly or laterally into the cavernous sinus [15,16].
We present a unique case of a giant pituitary metastasis from a duodenopancreatic Neuroendocrine Tumor (GEP-NETs), initially mistaken for a primary pituitary adenoma. We also aim to contextualize its clinical features, diagnostic process, and therapeutic considerations through a focused review of the existing literature. By highlighting both individual and collective experiences, we seek to improve recognition of this rare entity and support more informed clinical decision-making.
A 57-year-old male with no significant past medical history presented to the emergency department with a sudden onset of severe headache, vomiting, and progressive loss of consciousness. He was intubated for airway protection on arrival due to collapse. Initial CT imaging revealed a giant sellar lesion extending into the third ventricle, causing obstructive hydrocephalus (Figure 1). An emergent External Ventricular Drainage (EVD) was placed, and the patient was admitted to the Intensive Care Unit (ICU), where he was started on intravenous dexamethasone. Further systemic examination revealed an absence of body hair on the trunk and limbs, while facial and pubic hair remained intact. He exhibited no gynecomastia or galactorrhoea, and testicular volume was within normal limits. The family reported long-standing hair loss since adolescence, but had fathered four children by the age of 30. Laboratory investigations showed low levels of Follicle-Stimulating Hormone (FSH), Luteinizing Hormone (LH), testosterone, Growth Hormone (GH), and Free Thyroxine (FT4), with a normal Thyroid-Stimulating Hormone (TSH) level and Low Prolactin (PRL). He was started on levothyroxine for presumed central hypothyroidism.
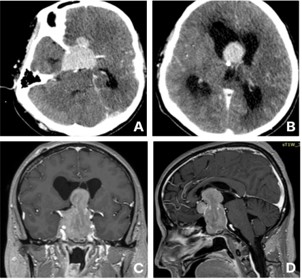
Figure 1: (A,B) Show axial cuts of the initial CT head post contrast. (C,D) Illustrate the lesion in the pre-op MRI in sagittal and coronal views.
MRI confirmed the presence of a giant sellar lesion extending into the suprasellar region and 3rd ventricle to the foramen of Monro (Figure 1). The lesion exhibited enhancement and diffusion restriction on Susceptibility-Weighted Imaging (SWI), with invasion of the bilateral cavernous sinuses and encasement of the internal carotid arteries. Also, the optic chiasm was compressed. In reduced sedation attempts, the patient was decerebrating.
Given the lesion’s size and intraventricular extension, the patient underwent pterional craniotomy for debulking as the first step of tumor excision. (Figure 2) shows the tumour debulking and the identification of the right Middle Cerebral Artery (MCA). As the MCA was promptly identified during the operation, local irrigation with papaverine solutions was applied. Postoperatively, the patient was transferred again to the ICU, and CT head showed the extent of debulking (Figure 3). Two days post-op, the patient developed anisocoria, and the repeated CT scan showed a right-sided MCA infarct with extensive midline shift (Figure 3). Despite intraoperative papaverine irrigation, significant MCA vasospasm was observed. Therefore, we did not continue with further endoscopic transsphenoidal resection. The patient subsequently succumbed to complications.
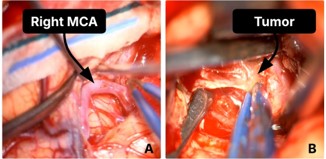
Figure 2: (A) Shows the right MCA identified intraoperatively, (B) Illustrates the lesion debulking.
Microscopically, the material consists of fragments of a cellular neoplasm with a predominantly nested growth pattern and a prominent vascular layer. The neoplastic cells in several locations are arranged around thin-walled, papillary vessels. The neoplastic cells are characterized by eosinophilic cytoplasm and relatively uniform nuclei with finely granular chromatin. ΑΕ1/ ΑΕ3 (+), INSM1 (+), GARA3 (+), CK19 (+), ISLE1 (+), 2-3 p53, Ki67 8%. Brain infiltrate from a NET G2. Histopathological examination of the tumor revealed features consistent with a neuroendocrine neoplasm (NET G2), with a presumed primary origin in the duodenum or pancreas.
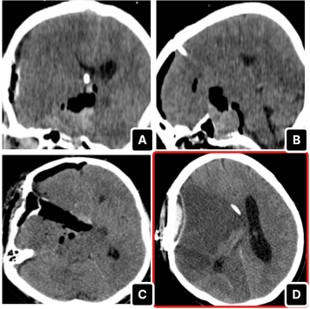
Figure 3: (A-C) show the immediate post-operative CT head, while (D) illustrates the right MCA infarct on day 2 post-op.
Literature review methodology
A focused literature review was conducted using the PubMed database (up to April 2025) to identify reported cases of pituitary metastases originating from gastrointestinal or pancreatic neuroendocrine tumors. Search terms included “pituitary metastasis,” “neuroendocrine tumor,” “pancreatic,” “duodenal,” “gastrointestinal,” and “sellar mass.” Only English-language case reports, case series, and reviews with histopathological confirmation were included. Studies lacking sufficient clinical or diagnostic data were excluded. Due to the rarity and heterogeneity of available data, findings are presented as a narrative synthesis rather than a formal systematic review.
The present case highlights a highly unusual presentation of a giant pituitary metastasis originating from a duodenopancreatic neuroendocrine tumor—an entity that remains exceptionally rare in the literature. Although the pituitary gland is an uncommon site for metastatic disease, the coexistence of a large sellar mass and the absence of a known primary malignancy at presentation significantly complicate the diagnostic process. In our case, the clinical, radiological, and endocrinological findings closely mimicked those of a benign pituitary macroadenoma, underscoring the difficulty of preoperative diagnosis. Definitive diagnosis was only established following surgical intervention and histopathological analysis.
Molecular background
Molecularly, pituitary metastasis is largely influenced by the tumor microenvironment, where vascular factors, hormone gradients, and immune infiltrates influence tumor seeding and proliferation [1]. For example, prolactin-rich settings may draw breast cancer cells to the pituitary, while Vascular Endothelial Growth Factor (VEGF) and hypoxic gradients can promote implantation [1]. Recent studies have demonstrated the oncogenic role of the Pituitary Tumor-Transforming Gene 1 (PTTG1) in promoting tumor invasiveness and metastasis across gastrointestinal malignancies, suggesting new possibilities for targeted diagnosis and treatment [17-19]. PTTG1 oncogene is found overexpressed in 60-66% of esophageal squamous cell carcinomas, correlating strongly with lymph node metastases and decreased survival [17,18]. The same marker of tumor aggressiveness has been observed in 65.3% of gastric carcinomas and is associated with metastasis [18,19].
Additionally, genetic syndromes such as MEN1 and MEN4, associated with mutations in MEN1 and CDKN1B, respectively, suggest a shared oncogenic pathway in endocrine and gastrointestinal malignancies [20-23]. Furthermore, historical studies have observed the loss of heterozygosity at chromosome 13q12-14, involving tumor suppressors such as RB1 and BRCA2, in 16% of parathyroid adenomas and some rare pituitary tumors, raising thoughts of a shared genetic vulnerability across endocrine neoplasms [21]. Lastly, pancreatic tumors that often express chromogranin A, synaptophysin, and Ki-67 can be differentiated histopathologically from primary pituitary adenomas [1,4].
Clinical characteristics
Clinical presentation of pituitary metastases varies based on tumor characteristics and biological behavior. Recent studies revealed that pituitary metastases often present with headache (67%), visual disturbances (86%), anterior hypopituitarism (71%), and diabetes insipidus (38%), the latter reflecting posterior lobe involvement due to its direct systemic blood supply [1,5,24-26]. Symptoms may mimic those of benign pituitary adenomas, complicating early diagnosis. Notably, diabetes insipidus remains the hallmark symptom and can aid in differentiating metastasis from benign adenomas [5]. In some rapidly developed cases, the mass effect was the reason for the presentation [27]. Given that over half of pituitary metastases are only diagnosed intraoperatively, diagnostic difficulties are further underlined [3].
MRI is the preferred imaging modality for diagnosing pituitary lesions. Radiologically, pituitary metastases often mimic adenomas with typical features of pituitary stalk thickening, sellar masses with suprasellar extension, homogeneous contrast enhancement, and cavernous sinus invasion [1,6,10]. Sometimes it can be suspected due to irregular margins and rapid tumor growth, especially in the absence of a known primary sellar lesion [7,24,28]. In fact, up to 24% of patients are diagnosed with pituitary metastasis before their primary malignancy is identified [24]. In rare cases, metastases can also be mistaken for aneurysms, further complicating the diagnosis [25].
Treatment strategies
Therapeutic management of pituitary metastases, particularly those from Neuroendocrine Tumors (NETs), requires a multimodal approach tailored to disease extent and tumor origin. Surgical resection, often via transsphenoidal route, is primarily used for symptom control, especially in cases of visual compromise or significant mass effect, and tissue diagnosis, with subtotal resection achieved in 76% of cases [24,25,27]. However, in cases involving extensive lateral extension, encasement of the internal carotid arteries, or fibrous tumor consistency, transcranial or staged combined approaches may be necessary [14,29]. For giant pituitary lesions similar to the current case, large case-series studies showed that gross total resection was achieved in 63.8% of cases, with postoperative visual improvement in nearly 79% of patients [15]. When anatomical complexity or tumor consistency precludes complete resection, partial debulking can still yield substantial symptom relief.
As sellar metastases often indicate an advanced systemic disease, surgery alone is rarely curative. Adjuvant radiation-including stereotactic radiosurgery and external beam therapyis frequently administered in about 67% of patients and leads to partial symptomatic relief [2,24]. Systemic therapy remains critical, particularly for patients with widespread disease or poor surgical candidacy, with median overall survival ranging from 12 to 25 months depending on histology and intervention [2,24,28]. For pituitary metastases from gastric cancer, regimens including oxaliplatin and fluoropyrimidines provide temporary disease control [7]. For the treatment of hypopituitarism and diabetic insipidus, hormonal replacement is essential. While dopamine agonists have demonstrated usefulness in regulating pancreatic polypeptide levels (Pathak et al., 2004), somatostatin analogs such as octreotide successfully decrease hormone release in NET-related instances [12,30]. Additionally, targeted therapies -including imatinib for GIST metastases and tyrosine kinase inhibitors like sorafeniboffer promising avenues for systemic control [26,27].
Histopathology
In order to distinguish metastases from primary pituitary adenomas, histopathological examination is essential [4,24]. The gastrointestinal origin was confirmed by reported examples of gastric cancer metastases to the pituitary that tested positive for CK7, CK20, CDX-2, and chromogranin A [7,10]. A high Ki-67 index also suggests an aggressive neoplastic process. Similarly, pituitary adenomas have been linked to neuroendocrine tumors that arise in MEN1 disease, such as thymic carcinoids, which raises concerns regarding hereditary risk [23]. Histologically, differentiating pituitary neuroendocrine tumors from metastatic neuroendocrine cancers can be challenging and often requires a complex panel of immunostains and correlation with primary tumor histology [31].
Prognosis
The overall prognosis of pituitary metastasis patients is poor, with a 71% mortality rate during a mean follow-up of 2.4 years [3]. More specifically, the prognosis for patients with gastric cancer metastasizing to the pituitary remains poor. Mortality is frequently due to broad metastatic disease rather than pituitary involvement alone, and reported survival rates are usually less than 12 months after diagnosis [10]. Crucially, surgical resection was associated with improved survival, particularly in patients under 60 and those with primaries other than lung or breast [2]. In contrast, patients with non-solitary pituitary metastasis or no local therapy had significantly worse survival outcomes [28].
To conclude, a rare case of giant pituitary metastasis from a duodenopancreatic neuroendocrine tumor is presented that was initially mistaken for a pituitary adenoma. Diagnostic difficulties persist due to the clinical and radiological similarities between primary pituitary tumors and metastases, especially when pituitary involvement occurs before the original cancer is discovered. The current case highlights how crucial it is to consider metastatic disease in the differential diagnosis of large or atypical sellar masses, particularly in cases of rapid neurological or endocrine profile deterioration. Histopathology is essential for a conclusive diagnosis. Given the typically poor prognosis despite intervention, timely diagnosis and a multidisciplinary approach are critical for optimizing outcomes and guiding appropriate therapeutic strategies.
To conclude, a rare case of giant pituitary metastasis from a duodenopancreatic neuroendocrine tumor is presented that was initially mistaken for a pituitary adenoma. Diagnostic difficulties persist due to the clinical and radiological similarities between primary pituitary tumors and metastases, especially when pituitary involvement occurs before the original cancer is discovered. The current case highlights how crucial it is to consider metastatic disease in the differential diagnosis of large or atypical sellar masses, particularly in cases of rapid neurological or endocrine profile deterioration. Histopathology is essential for a conclusive diagnosis. Given the typically poor prognosis despite intervention, timely diagnosis and a multidisciplinary approach are critical for optimizing outcomes and guiding appropriate therapeutic strategies.
Ethics statement: Written informed consent was obtained from the patient’s next of kin for publication of this case report and accompanying images.
Acknowledgment: The authors declare that there are no acknowledgements to disclose.
Funding sources: This research did not receive any specific grant from funding agencies in the public, commercial, or notfor-profit sectors.