Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Rupayan Kundu
Resident, Department of Internal Medicine, Cleveland Clinic Foundation, Cleveland, OH, USA.
Email: kundur2@ccf.org
Received: Mar 05, 2026 Accepted: Apr 06, 2026 Published: Apr 13, 2026
Citation: Batra H, Kasera A, Prasad A, Yadav A, Kundu R, et al. Acute ruptured hemorrhagic ovarian cyst: CT findings in a life threatening presentation. Ann Case Rep Med Images. 2026; 3(1): 1081.
Copyright: Kundu R et al. © All rights are reserved
Background: Though infrequently encountered, a ruptured hemorrhagic ovarian cyst can cause sudden, severe abdominal pain and can be mistaken for other emergency gynecologic or abdominal conditions.
Case report: A 36-year-old woman presented with acute onset severe abdominal pain with vomiting and a sudden and deteriorated with significant drop in hemoglobin. Ultrasound revealed a heterogeneous pelvic mass with free fluid, and the right ovary could not be visualized separately. A contrast-enhanced CT scan demonstrated a large adnexal cystic lesion containing hyperdense intralesional hemorrhage (approximately 60 HU) with moderate hemoperitoneum. No torsed pedicle was identified. Patient underwent emergency laparotomy which confirmed a ruptured hemorrhagic ovarian cyst with large-volume hemoperitoneum. Postoperatively, the patient recovered well.
Conclusions: CT is valuable when ultrasound findings are inconclusive. It provides essential information regarding source of hemorrhage, organ of origin of the lesion and any associated complications, guiding us for a timely surgical decision.
Keywords: CT imaging; Hemoperitoneum; Hemorrhagic ovarian cyst; Adnexal mass; Acute abdomen.
Hemorrhagic ovarian cysts commonly arise from functional cysts, following intracystic hemorrhage and in majority of patients resolve spontaneously [1]. However, rupture though uncommon presentation is clinically significant as it can lead to acute abdomen and significant hemoperitoneum, requiring prompt recognition [2]. Ultrasound remains the initial tool used for investigation in acute pelvic pain in reproductive age women but may be limited by interobserver variability and technical limitations such as distorted pelvic anatomy as in large abdomino-pelvic lesions where adnexal origin cannot be determined with certainty and poor visualization due to large-volume hemorrhage. In such cases, Contrast Enhanced Computed Tomography (CECT) provides critical information regarding the origin of the lesion being adnexal, the extent of hemoperitoneum and ruling out close mimics like adnexal torsion, ovarian malignancy, other causes of acute pelvic pain [3].
Clinical presentation and history
A 36-year-old woman was in perfect health, suddenly presented with lower abdominal pain which was progressive in nature, severe in intensity associated with bilious vomiting. The past history was significant for cholelithiasis and irregular menstruation.
In the day following, she became tachycardic and visibly distressed. Initial laboratory evaluation was done, routine blood tests were ordered like complete blood count, liver function test, kidney function test etc and revealed a profound drop in hemoglobin to 4 g/dL. The urine pregnancy test was negative.
Imaging findings
Ultrasound demonstrated a heterogeneously hypoechoic pelvic mass with free intraperitoneal fluid that had echoes within. The right ovary could not be identified separately from the lesion, and provisional considerations included ovarian torsion or a ruptured hemorrhagic cyst.
To further characterize the lesion, an urgent contrast- enhanced CT scan was performed. Non-contrast images showed a large adnexal cystic lesion containing hyperdense hemorrhage (approximately 60 HU) (Figure 1). Portal venous phase images demonstrated internal clots and minimal peripheral enhancement and a region of irregularity was also noted in the left lateral wall. No torsed pedicle or evidence of active contrast extravasation was seen. Moderate hemoperitoneum extended into the pelvis, paracolic gutters, and Morrison’s pouch (Figures 2 and 3).
Given the patient’s hemodynamic instability and rapid hemoglobin decline, she underwent emergency exploratory laparotomy. Intraoperatively, a ruptured hemorrhagic ovarian cyst with extensive hemoperitoneum was identified and excised. The patient remained stable postoperatively and was discharged after 3-4 days.
Intra-operative and surgical findings
Emergency exploratory laparotomy was undertaken in view of hemodynamic instability and a rapid decline in hemoglobin levels. On opening the abdomen, a large volume of hemoperitoneum was encountered, consisting of fresh and partially clotted blood occupying the pelvis and upper abdomen.
The right ovary was found to be enlarged and distorted by a ruptured hemorrhagic cyst. An irregular rent was noted along the lateral cyst wall with active oozing of blood (Figure 4). No evidence of ovarian torsion, twisted vascular pedicle, or ischemic change was identified.
The cyst cavity contained organized clots and altered blood products, correlating with the hyperdense intracystic hemorrhage seen on preoperative CT. Active pelvic bleeding from the rupture site accounted for the extensive hemoperitoneum (Figure 5).
The uterus and contralateral ovary appeared grossly normal, with no features suggestive of malignancy, endometriosis, or pelvic inflammatory disease. The ruptured cyst was excised, hemostasis was secured, and thorough peritoneal lavage was performed.
Hemorrhagic ovarian cysts represent a common functional adnexal pathology, but rupture is unlikely and even more rare is its acute abdomen presentation with significant fall in hemoglobin. When associated with hemoperitoneum, the acute presentation constitutes a true gynecologic emergency that requires early and accurate diagnosis [4].
Imaging modalities and their roles
Ultrasound is the first line modality for evaluating acute abdomen in a young female of reproductive with the major advantage being its availability, examining in the real time and the the absence of ionizing radiation [5].
However, findings may be nonspecific, especially in the presence of such a large sized mass lesion with abdominal extension making it difficult to realize the adnexal origin, especially to identify that the wall complicating to make a diagnosis of ovarian cyst rupture. Large-volume hemoperitoneum further complicates the evaluation [6]. In such difficult setting, CT becomes invaluable for suggesting adnexal origin of the lesion, its relationship with surrounding structures, the presence of hyperdense intralesional blood. It also helps in ruling out rupture by identifying discontinuity and irregularity of the wall and assessing the extent and distribution of hemoperitoneum [7]. CT is also the key tool in ruling out potential mimics like ovarian torsion which is the most common cause of sudden onset pain in young female and is one of the most common pelvic emergency requiring prompt recognition and treatment. It aids in identifying enlarged ovary with peripheral follicles, midline location and torsed vascular pedicle [8].
Clinical and radiological differentials and their distinguishing points
Imaging aids in identifying enlarged ovary with peripheral follicles, midline location and torsed vascular pedicle [8]. Another mimic of hemorrhagic cyst can be adnexal neoplasms causing intralesional hemorrhage can also be well evaluated on CT by identification of the solid enhancing components, papillary projections, irregular wall, peritoneal nodules, all of these features are typically absent in hemorrhagic cyst.
| Condition | Clinical features | Ultrasound findings | CT imaging features | Distinguishing points |
|---|---|---|---|---|
| Ruptured hemorrhagic ovarian cyst [2-4] | Sudden onset severe lower abdominal pain; may present with hemodynamic instability and acute hemoglobin drop; negative pregnancy test | Complex cyst with internal echoes; free fluid with low-level echoes; ovary may not be separately visualized | Hyperdense intracystic hemorrhage (50-70 HU); internal clot; thin minimally enhancing wall; focal wall irregularity or discontinuity; moderate to large hemoperitoneum | Adnexal origin, hyperdense intralesional blood, absence of solid enhancing components and torsed pedicle |
| Ovarian torsion [6,8,9] | Acute pelvic pain with nausea and vomiting | Enlarged ovary with peripheral follicles; reduced or absent Doppler flow | Enlarged ovary; peripheral follicles; twisted vascular pedicle (“whirlpool sign”); midline displacement; minimal hemoperitoneum | Visualization of torsed pedicle and ovarian enlargement without intracystic hemorrhage |
| Adnexal neoplasm with hemorrhage [10,11] | Subacute or chronic pain; possible abdominal distension or weight loss | Complex solid–cystic mass | Solid enhancing components; papillary projections; thick irregular wall; peritoneal nodules or ascites | Presence of enhancing solid tissue and malignant morphological features |
| Ruptured ectopic pregnancy [6,9,12] | Acute abdominal pain; amenorrhea; hemodynamic instability; positive β-hCG | Empty uterus; adnexal mass; free fluid | Hemoperitoneum; adnexal mass without ovarian morphology | Positive pregnancy test and absence of ovarian cyst wall |

Figure 1: Non-contrast axial CT showing a cystic right adnexal lesion with hyperdense hemorrhage and associated pelvic free fluid.
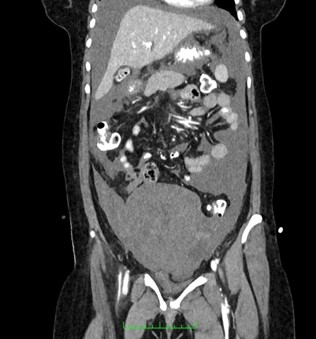
Figure 2: Coronal portal venous phase CT demonstrating the vertical extent of the adnexal cystic lesion and hemoperitoneum.
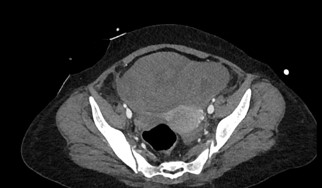
Figure 3: Axial portal venous phase CT showing internal clot and a thin, minimally enhancing cyst wall.

Figure 4: Intraoperative specimen of the ruptured hemorrhagic ovarian cyst with adherent clots.
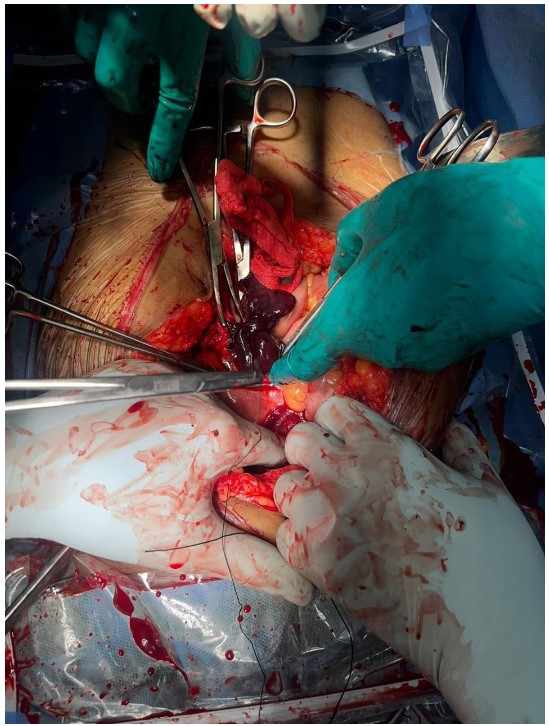
Figure 5: Intraoperative photograph showing hemoperitoneum and active pelvic bleeding.
Treatment and surgical approach
The management of hemorrhagic ovarian cysts is guided by the patient’s clinical condition, severity of symptoms, and the presence of associated complications. In hemodynamically stable patients with mild symptoms, conservative treatment with analgesia and close clinical and imaging follow-up is usually sufficient, as most functional hemorrhagic cysts resolve spontaneously [2].
Surgical intervention is indicated in patients with persistent or worsening pain, diagnostic uncertainty, significant hemoperitoneum, or hemodynamic compromise. The aim of surgery is control of bleeding with maximal preservation of ovarian tissue. Laparoscopy is preferred in stable patients; however, laparotomy may be required in cases of massive intraperitoneal hemorrhage or rapid clinical deterioration.
In the present case, the patient developed acute hemodynamic instability accompanied by a profound drop in hemoglobin levels and imaging evidence of extensive hemoperitoneum. Given the life-threatening presentation, emergency exploratory laparotomy was performed. A ruptured hemorrhagic ovarian cyst with active bleeding was identified and excised, hemostasis was secured, and peritoneal lavage was carried out. The postoperative course was uneventful [4].
Postoperative imaging and follow-up
Follow-up ultrasonography showed mild free fluid in the peritoneum with no residual adnexal lesion. The patient remained clinically stable with improving hemoglobin levels and was discharged after 4 days with no fresh complaints at the time of discharge.
CT plays an indispensable role in evaluating acute pelvic emergencies especially when first line investigations like ultrasound are inconclusive [9]. Recognizing adnexal origin of lesion, identifying rupture in ovarian cystic lesions, demonstrating hyperdense internal clot and extent of hemoperitoneum enables timely diagnosis and appropriate intervention, reducing morbidity and mortality leading to a delayed treatment.
Author contributions: Himanshi Batra: Conceptualization, imaging interpretation, manuscript drafting; Anmol Kasera: Data collection, manuscript drafting, collection of images; Rupayan Kundu: Data collection, manuscript drafting, critical revision; Akhila Prasad: Supervision, critical revision, final approval; Akanksha Yadav: Data collection, imaging interpretation; Ankit Batra: Data collection, manuscript preparation.
Conflict of interest statement: The authors declare that there are no conflicts of interest regarding the publication of this paper.
Funding statement: No funding was received for this study.
Ethical approval: This case report was conducted in accordance with institutional ethical standards. As this is a single case report with anonymized patient data, formal ethical committee approval was not required as per institutional policy.
Patient consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the consent is available for review by the Editor-in-Chief upon request.
Acknowledgement: The authors would like to thank the Department of Radiodiagnosis, Dr. RML and ABVIMS Hospital, New Delhi, for their support in the preparation of this manuscript.
Data availability statement: All relevant data supporting the findings of this study are included within the article. Additional details are available from the corresponding author upon reasonable request.
Guarantor of submission: Dr. Rupayan Kundu accepts full responsibility for the integrity of the work as a whole.
Key clinical message: Although hemorrhagic ovarian cysts are usually self-limiting, rupture may occasionally lead to massive hemoperitoneum and hemodynamic instability. In such situations, timely CT evaluation is essential to establish the diagnosis, exclude other surgical emergencies, and facilitate prompt management.