Article Type: Research Article, Volume 3 Issue 1
*Corresponding author: Sijia Na
Department of Oral and Maxillofacial Surgery, Key Labora tory of Shaanxi Province for Craniofacial Precision Medicine Research, College of Stomatology, Xi’an Jiaotong University, Xi’an, China.
Email: sijiana@xjtu.edu
Received: Mar 11, 2026 Accepted: Apr 03, 2026 Published: Apr 10, 2026
Citation: Xie L, Ahmadi S, Lv C, Tu J, Na S, et al. Supernumerary teeth extraction via robot-assisted surgery without flap elevation. Ann Case Rep Med Images. 2026; 3(1): 1080.
Copyright: Na S et al. © All rights are reserved
Background: Impacted supernumerary teeth often require surgical intervention, which may involve extensive bone removal and risk to adjacent anatomical structures. Minimally invasive techniques, especially those facilitated by robotic technology, provide a viable alternative.
Objective: To assess the clinical feasibility, safety, and short-term effects of robot-assisted minimally invasive extraction of impacted supernumerary teeth without flap elevation.
Methods: A total of 4 patients underwent removal of impacted supernumerary teeth using a computer-guided navigation system with robot-assisted tooth extraction. Preoperative planning consisted of Cone-Beam Computed Tomography (CBCT) to aid the surgeon in locating essential anatomical structures. All procedures were completed under local anesthesia with postoperative follow-up at days 1, 7, and 30. Feasibility outcome measures included procedural completion rates, intraoperative navigation accuracy, and the extent to which the surgeon could modify the robotically assisted surgical plan.
Results: All procedures were completed with a mean operative time of 10±5 minutes. No intraoperative complications, including hemorrhage, edema, sinus fistula, nerve damage or adjacent teeth damage, were observed. Postoperative follow-ups confirmed rapid wound healing and absence of adverse events. Patients reported high satisfaction in terms of comfort and esthetic outcomes.
Conclusion: Robot-assisted flapless extraction is a safe, efficient, and patient-centered technique for the removal of impacted supernumerary teeth. It shows strong potential to reduce surgical trauma and improve recovery compared to conventional methods.
Keywords: Robot-assisted surgery; Flapless extraction; Impacted supernumerary teeth.
Supernumerary Teeth (ST) are anomalies of development defined as the presence of additional teeth beyond those dictated by the typical dental formula. They may be located at any site in the jaws, but most often appear in the maxillary anterior region, thus causing clinical sequelae such as impaction, displacement of adjacent teeth, or cyst formation [1,2]. Their management as impacted supernumerary teeth creates a significant challenge in oral and maxillofacial surgery because of their erratic positioning, proximity to vital structures (e.g., nerves, roots of adjacent teeth), and their capacity for occlusal disharmony [3,4]. Hidden teeth, whether supernumerary or of normal origin, can set forth a chain of pathological events, including pericoronitis, root resorption, odontogenic cysts, or inhibiting the eruption of permanent teeth [5,6]. The situation necessitates surgical extraction, but conventional methods involving extensive osteotomy carry the risk of nerve injury, loss of alveolar bone, and postoperative morbidity [7,8].
To date, a conclusive surgical approach for extracting impacted teeth that minimizes postoperative complications has not been determined [9]. One such method is the bone lid, developed for maxillary sinus procedures and apical root resections [10,11]. This involves making a cortical bone window (or “lid”) that is temporarily lifted to assess the surgical site, then replaced to minimize osseous injury and allow healing. The bone lid method has been adapted for the extraction of impacted teeth requiring more specific anatomical preservation and approaches, for example, the mandibular ramus or posterior maxilla [12-14]. Nevertheless, the disadvantages of the bone lid method include flap elevation and manual osteotomy, both of which are more invasive and time-consuming than other, more conservative methods [14]. To address this challenge, this study explored a flapless robot-assisted minimally invasive surgical technique. By combining navigation and positioning with minimally invasive K-wire and drilling techniques, it aims to achieve the same or even better surgical field exposure while minimizing damage to bone and soft tissues.
Digital robots have been utilized in various fields, including oral surgery, the treatment of head and neck tumors, oral implants, and endodontic procedures. These robots offer a range of benefits, such as improved precision, enhanced safety, freedom from visibility limitations, and greater adaptability [15]. Autonomous robots are especially suitable for activities that demand accurate alignment and consistent performance, assisting surgeons in minimizing manual errors and reducing the risk of complications [16,17]. Furthermore, robot-assisted surgery offers advantages such as real-time feedback and tactile constraints, making it a viable alternative to conventional guided alveolar surgery. Retana et al. [3] successfully performed several minimally invasive extractions of impacted supernumerary teeth using dynamic navigation technology, and follow-up 1 week later showed good wound healing. [3] Han et al. [18] reported three cases of robot-assisted minimally invasive extraction of impacted teeth, and follow-up one month later showed good healing results in all cases [18].
This paper presents four clinical case studies focusing on the minimally invasive extraction of impacted supernumerary teeth using intelligent digital robotic systems. These robotic units operate independently while remaining under the supervision of dental surgeons to ensure precision and safety. This research aims to evaluate the practical benefits of employing autonomous robotic technology in the surgical management of supernumerary teeth, thereby contributing valuable insights and reference data to advance clinical applications.
Clinical report
There were four patients that had minimally invasive extraction of supernumerary teeth that were impacted at the Outpatient Clinic of Oral and Maxillofacial Surgery of the Affiliated Stomatological Hospital of Xi’an Jiaotong University. Preoperative systemic evaluation in addition to specialized examination was made by Dr. L.X. and L.C.P. The patient population represents patients who have excellent systemic health and no history of systemic disorders, nor hereditary disorders in their family histories. Table 1 shows the clinical characteristics of the four patients.
Preoperative preparation and surgical planning
Before the surgical procedure, a flowable restorative material (3M, Z350XT) was employed to secure the marker to the teeth in the non-surgical region of the maxilla (Figure 2A-D, Figure 3A).
Data in the Digital Imaging and Communications in Medicine (DICOM) format were acquired using Cone-Beam Computed Tomography (CBCT, Planmeca) and then analyzed using robot software (RemebotDent, v1.0.0.2; Beijing) for surgical planning and three-dimensional reconstruction of the impacted supernumerary teeth (Figure 2A-D, Figure 1A-C). The red outline designates the surgical field where intervention would take place to allow for accurate preoperative planning. This completed planning indicated what specific paths the various drills would travel during the surgical procedure. These paths were mapped out to ensure the highest accuracy is achieved throughout the osteotomy portion of the procedure.
The drilling protocol (Table 2) was followed in a stepwise manner to confirm that the osteotomy was completed correctly at every stage, from initial markings to final widening, along the intended drill paths.
A cylindrical simulated item was built on the computer and drilled with dimensions marginally above the distance between the jaw surface and the affected tooth, together with a diameter beyond the maximum circumference of the dental crown. The physician verified the drill’s definitive placement.
The marker affixed to the teeth comprised seven magnetic beads that were discernible in the CBCT imaging data. The primary role of the marker is to execute registration and calibration in surgical preparation, as well as to assist in robot placement and tracking during surgical procedures (Figure 2D).
Registration and calibration
On the day of surgery, local anesthesia was administered to the patient followed by standardized sterilization of the maxillofacial region and oral cavity. The navigation program was initiated using a visible-light optical locator (Remebot, Beijing, China), followed by sequential registration and calibration of the marker and calibration plate. The robot’s product specification indicates that the calibration plate was placed in the frontal region (about four fingers above the tip of the nose), the left cheek (approximately at the left molar position), and the right cheek (approximately at the proper molar position), ensuring alignment with the marker (Figure 3B).
The surgical plan was precisely executed during the procedure using real-time navigation. The drill paths were executed under robotic guidance, ensuring minimal deviation from the preoperative plan. The navigation system continuously monitored the robotic arm’s position and made real-time adjustments to compensate for any displacement.
The drilling protocol, as outlined step-by-step in (Table 2), ensured that each stage of osteotomy—from initial marking to final widening—was completed with precision, following the planned drill trajectories.
Surgical procedure
Before the procedure, the patient is fitted with markers for CBCT scanning, allowing the software to autonomously reconstruct the oral dentition, alveolar bone, neural canal, maxillary sinus, and additional structures, thereby facilitating the formulation of surgical plans for the clinicians. The optical tracking and positioning equipment collects the positions of the robotic arm and the patient in real time, immediately and accurately detects any tiny displacement of the patient, and calibrates the robotic arm to the correct initial position. Then, the robotic arm accurately reaches the prepared position. The doctor pushes the gripper in the direction limited by the robot, which guides the drill needle to the extraction position accurately, and, with the help of different drill needles, completes extraction site positioning, hole preparation, tooth exploration, and other operations (Figure 2D).
The procedure was performed as robot-assisted minimally invasive surgery, eliminating the need for flap elevation or a sterile steel scalpel. With detailed preoperative planning, the robotic system created a precise, minimally invasive access point through the palatal mucosa, preserving surrounding soft tissues. This minimally invasive approach significantly reduced surgical trauma and promoted accelerated postoperative healing.
A triangular drill was mounted on the robotic manipulator, which autonomously navigated to the predefined surgical coordinates to mark the cortical bone and verify trajectory alignment (Figure 2E). Following this confirmation, the robotic system proceeded with the sequential osteotomy preparation using a series of calibrated drills, as visually documented in (Figure 2F-H).
The osteotomy began with the triangular drill (2.0-3.3 mm), which initiated cortical entry and established the intended drill trajectory. This was followed by the round drill (1.4-3.4 mm), penetrating the cortical plate to a depth of 4 mm. A second-round drill (2.3-3.4 mm) was then employed to deepen the osteotomy to 7 mm, allowing further canal formation. Subsequently, the pilot drill (2.2-4.1 mm) was introduced to prepare the full-length osteotomy at 10 mm depth (Figure 3C). This was followed by the reamer drill (3.5-4.1 mm) for pre-final canal shaping, and finally, a larger reamer drill (4.2-4.1 mm) was used to complete the osteotomy with the desired geometry (Figure 3D). The drilling protocol is shown step-by-step in (Table 2).
Each drill was precisely positioned by the robotic system, operating under continuous irrigation to prevent thermal injury.
The implant system was operated at 1500 rpm for tooth splitting and osteotomy. This speed provided sufficient cutting efficiency while minimizing heat generation and trauma to surrounding tissues. All drills, including triangular, round, pilot, and reamer types, were utilized under this standard speed setting to ensure consistency and procedural safety.
The surgeon actively monitored the intraoperative field and robotic interface in real time to ensure safety and accuracy throughout the procedure.
Once the osteotomy was completed, the impacted supernumerary teeth were exposed through the minimal access created. The surgeon proceeded with the manual extraction of the teeth. Depending on anatomical complexity, a dental elevator was employed for luxation. Hemostatic forceps were utilized to facilitate the removal of the loosened teeth (Figures 3E-G).
As demonstrated in the aforementioned steps, robot-assisted flapless extraction enables precise localization of impacted teeth and achieves accurate bone removal and tooth segmentation. Even in complex anatomical scenarios, it ensures efficient completion of the final stage of tooth division while avoiding additional tissue damage.
After the procedure, the access site was closed carefully with CGF and a gelatin sponge to ensure primary closure, minimizing tissue trauma and promoting efficient postoperative recovery (Figures 3H-J).

Figure 1: Overview of the clinical workflow: (A) Clinical Experimental Procedure. (B) Main components of the robotic assisted system. (C). Diagram of the Surgical Model.

Figure 2: The position of supernumerary teeth (ST) in CBCT and preoperative planning strategies within the robotic operating system. (A-D) Preoperative 3D (CBCT) imaging provides a comprehensive view of the patient’s dental anatomy. The impacted ST was located on the palatal side of teeth 21 and 22 in the maxillary bone. During the surgical planning stage, the CBCT images were overlaid with a blue digital model of the robotic system. The red outline indicates the target area for surgical intervention, facilitating accurate preoperative planning. (E-H) Drilling Protocol Step-by-Step: 1. Pre-drilling/positioning phase: a triangular drill (drill size: 2.0-3.3 mm) used for initial osteotomy. 2. The second step of guided osteotomy, using a round drill sized 1.4-3.4 mm, reached a depth of 2 mm. (Osteotomy completed) indicator is green for 2.0 mm → suggesting the initial cortical entry is complete. 3. Osteotomy expansion: Progressing through the osteotomy sequence confirms that osteotomy at 7.0 mm depth is complete. 4. Pilot drills: Initial full-length osteotomy (2.2-4.1 diameter) and the final (2.8-4.1 diameter) osteotomy depth reached 10 mm. 5. Final osteotomy widening steps: A progressive 3.5 mm drill followed by a 4.2 mm drill, both to 10 mm depth. (All drills were in preparation for the Straumann 4.8×10 mm implant.)
Postoperative care
Prophylactic antibiotics were supplied to avert postoperative infections at the surgical site. The patient concurrently gargled and washed his mouth with a povidone-iodine solution.
Four minimally invasive extractions of impacted supernumerary teeth with robotic assistance were successfully performed. The average operation duration was 10 minutes ± 5 minutes. One day post-surgery, there was an absence of bleeding or edema at the surgical site, and no problems such as maxillary sinus fistula, oral-nasal communication, nerve injury, or adjacent teeth damage were seen. At the follow-up appointments one week and one-month post-surgery (Figure 3J), the patient’s wound showed satisfactory healing, and the patient expressed high satisfaction with the use of this technique (Figure 4).
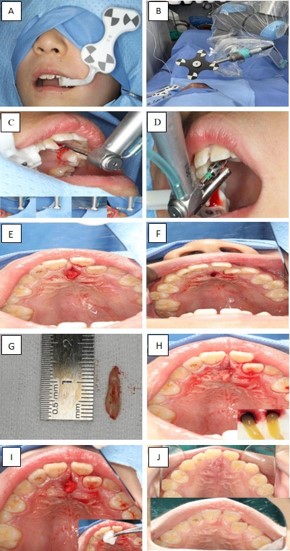
Figure 3: Surgical procedure. (A) Patient setup with a marker attached to the maxillary region in contralateral teeth. (B) The calibration plate is positioned on the left cheek (approximate left molar position) to align with the marker. (C) A ball drill locates surgery’s first step. Includes step-by-step explanations of the procedure’s burs, as shown in the smaller images (Table 1). (D) A close-up image of the ring drill partially removes bone. (E) An intraoperative view reveals the surgical site after the osteotomy with ST. (F) Surgical site post-osteotomy. (G) The removed ST is shown next to a ruler to illustrate its dimensions. (H-I) Concentrated Growth Factor (CGF) and a collagen sponge were applied. (J) The final image after surgery shows the fully healed surgical site, with the one-week follow-up on top and the one-month follow-up on the bottom, indicating that the soft tissue is well-aligned and free from complications.
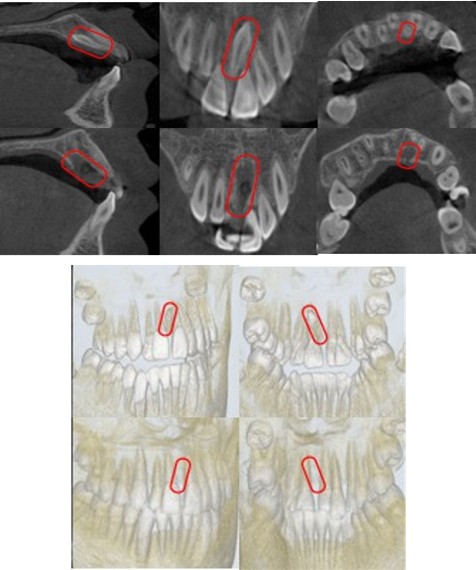
Figure 4:CBCT images of the Supernumerary Teeth (ST) position and orientation.The ST is impacted palatally between the maxillary central incisors, oriented in an inverted position. Top row: Preoperative CBCT views. From left to right, there are sagittal, coronal, axial, and 3D volume-rendered reconstructions (frontal and oblique views). Bottom row: Immediate Postoperative CBCT views showing the surgical site after removal of the ST. The red outline indicates the location of the ST in the preoperative images and the corresponding area in the postoperative scans.
| Number | Gender | Age | General condition | Impacted tooth position | Flap elevation | Clinical diagnosis | Operative time (min) | Complication | Wound healing |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 8 | No systemic illnesses | Maxillary anterior region | No | Impacted supernumerary tooth | 15 | No | Exellent |
| 2 | Female | 8 | No systemic illnesses | Maxillary anterior region | No | Impacted supernumerary tooth | 12 | No | Exellent |
| 3 | Male | 8 | No systemic illnesses | Maxillary anterior region | No | Impacted supernumerary tooth | 11 | No | Exellent |
| 4 | Male | 9 | No systemic illnesses | Maxillary anterior region | No | Impacted supernumerary tooth | 14 | No | Exellent |
| Step | Drill Type | Diameter (mm) | Drill tip | Depth (mm) | Notes |
|---|---|---|---|---|---|
| 1 | Triangular drill | 2.0-3.3 | 0 | 0 | Triangular drill – initial marking |
| 2 | Round drill | 1.4-3.4 | 0 | 4 | Cortical entry |
| 3 | Round drill | 2.3-3.4 | 0 | 4 | Osteotomy expansion |
| 4 | Round drill | 2.3-3.4 | 0 | 7 | Deeper penetration |
| 5 | Pilot drill | 2.2-4.1 | 0.4 | 10 | First full-length preparation |
| 6 | Pilot drill | 2.8-4.1 | 0.4 | 10 | Intermediate finalization |
| 7 | Reamer drill | 3.5-4.1 | 0.4 | 10 | Pre-final drill |
| 8 | Reamer drill | 4.2-4.1 | 0.4 | 10 | Final osteotomy before implant |
Impacted supernumerary teeth are those that stay completely encased in the jaw for a lengthy duration and cannot erupt properly [6,19]. Due to their location in the jaw, they may be impeded by adjacent teeth, soft tissue, and osseous tissue. This frequently results in lesions or displacement of neighboring teeth, obstructing normal tooth eruption and inducing alveolar bone resorption. Moreover, impacted supernumerary teeth can lead to the development of odontogenic diseases, increasing the risk of cysts and oral infections and thereby significantly diminishing the patient’s quality of life [20-22]. Consequently, it is essential to eliminate the affected teeth and address pertinent clinical symptoms that immediately affect the neighboring teeth to improve the patient’s clinical condition.
Due to the resistance posed by soft tissue, osseous tissue, neighboring teeth, the inferior alveolar nerve canal, and the maxillary sinus cavity, along with the unique anatomical positioning of the oral cavity, it is imperative to adequately expose impacted supernumerary teeth during the extraction procedure to avert harm to the surrounding soft and hard tissues, as well as critical blood vessels and nerves [23]. This approach may result in consequences, including significant trauma, postoperative edema, and wound infection [24]. Conventional methods for addressing severely impacted or ectopic teeth—such as those located in the mandibular ramus, maxillary sinus, or lingual plate typically need significant flap elevation, bone excision, and soft tissue alteration [25,26]. These procedures not only prolong operational duration and elevate intraoperative hemorrhage but also lead to postoperative problems, including pain, edema, and neurosensory abnormalities [26]. Conversely, robotic-assisted minimally invasive surgery is a whole new approach: it utilizes superior visualization, tremor reduction, or improved instrument movement to precisely find and remove hidden teeth while being careful of the surrounding anatomical structures [27]. To achieve the objectives of precise osteotomy, tooth sectioning, and removal of the affected tooth with minimal tissue damage [18]. The growing prevalence of minimally invasive tooth extraction has prompted inquiries into improving precision, reducing surgical complexity, minimizing stress on the operative site, and minimizing complications associated with the procedure. Oral alveolar surgeons have aggressively addressed this significant clinical problem. The use of advanced technologies and techniques, including high-speed turbine handpieces, piezosurgery, and digital guidance, has markedly improved the precision, safety, and extent of trauma associated with these procedures. The advent of high-speed turbine handpieces has obviated the necessity for conventional intrusive bone removal techniques, which entail significant dangers and frequently result in various severe postoperative sequelae. Piezosurgery provides the benefit of selective cutting, which diminishes bone trauma from high-speed friction and minimizes nerve injury, as well as postoperative edema and discomfort [13]. Significantly, robotic aid facilitated real-time navigation and precise micro-movements, enabling targeted osteotomy and atraumatic tooth extraction. The use of preoperative Cone-Beam Computed Tomography (CBCT) with intraoperative robotic guidance significantly improved safety by providing precise spatial orientation and safeguarding vital tissues, including the inferior alveolar nerve, maxillary sinus floor, and neighboring roots [15,28].
This exploratory clinical experiment demonstrated that robot-assisted minimally invasive extraction of impacted supernumerary teeth can be performed in all four patients without flap elevation. The average operational duration was 10±5 minutes, indicating a substantial decrease compared to traditional methods [29]. Our method probably helped the healing process go so well since it was shorter and didn’t need flap elevation. Postoperative assessments conducted one day post-surgery indicated an absence of hemorrhage, edema, maxillary sinus fistula, nerve damage, or adjacent teeth damage. Subsequent evaluations, conducted 1 week and 1 month after the initial procedure, revealed complete wound healing and exceptional tissue regeneration, with no complications noted. Patients reported high satisfaction with aesthetic and functional outcomes. These findings highlight the capability of robot-assisted microsurgery to improve surgical accuracy, reduce trauma, and facilitate postoperative recovery in the treatment of impacted supernumerary teeth.
Beyond technical achievement, patient safety is crucial, especially in pediatric robotic surgery. For safe robot-assisted extraction, pediatric patients must remain still. Local anesthesia reduces the risks of anesthesia for pediatric patients and makes the procedure more convenient for them. Significant movement can affect operation accuracy and safety [27]. Advanced robotic systems use motion tracking and safety interlocks to prevent accidents. Dental robotic systems use visual tracking markers and sensors to monitor patient movement and correct the robot arm in real time. The robot’s “position-following” capacity lets it adapt to slight movements in real time and keep its position. The surgeon also continuously controls the system. The surgeon can stop motion at predictable measurements, and the robot can be trained to function only on foot pedal activation [27] Thus, if the patient moves unexpectedly, the robot can stop instantly. When treating young children with limited anatomy and low cooperation, these safety aspects are crucial. Robotic precision and fail-safes can be used for safe pediatric procedures to maintain the child’s composure during anesthesia. Combining a flapless, robot-assisted treatment with less surgical trauma for children reduces postoperative pain and swelling, preserves growing oral tissues, speeds recovery, and reduces psychological stress.
It is essential to investigate robot-assisted surgery to identify innovative, less invasive, safe, and easy techniques for the extraction of impacted supernumerary teeth. Robot-assisted operations have become increasingly common and are the subject of global study. Surgical robotic technologies mitigate the constraints of human motor abilities, providing precise motion control, high operational accuracy, excellent repeatability, and stability [30]. At now, robot-assisted surgery is progressively being used in diverse domains like dental implantology [31], urology [32], and cancer [33,34]. The implant robot’s high-precision positioning guarantees correct implantation angles and depths, as well as long-term stability [35]. Moreover, computer-assisted implant surgery offers enhanced precision, improved surgical success rates, and reduced operating durations compared to conventional techniques [15]. Moreover, extending robotic manipulators to other surgical and nonsurgical applications might enhance the applicability and benefits of these systems to meet the distinct requirements of various illnesses. Advancements in machine learning and artificial intelligence present prospective prospects for autonomous robotic surgical applications [36].
Despite the favorable results, this study is limited by its small sample size and the absence of a control group for comparison with traditional surgical methods. The brief follow-up duration limits the evaluation of long-term outcomes, including bone remodeling and any subsequent consequences. Moreover, the cost-effectiveness and accessibility of robotic systems remain unresolved challenges that may hinder their wider clinical implementation.
Subsequent research should include larger, multicenter randomized controlled trials to corroborate these initial findings and develop standardized techniques for robotic-assisted extraction of impacted supernumerary teeth. Longitudinal data on neurosensory preservation, osseous healing dynamics, and patient-reported outcomes will be crucial. The use of artificial intelligence in surgical planning and intraoperative guidance may improve procedural precision and independence, promoting broader clinical application.
Robot-assisted minimally invasive surgery is an innovative, accurate, and efficient method for removing impacted supernumerary teeth, providing improved safety, reduced tissue damage, and expedited recovery. Despite the limited current data, the use of robotic systems in oral and maxillofacial surgery might revolutionize conventional surgical practices, necessitating further clinical research.
Ethical declaration and informed consent: This study was approved by the Institutional Review Board of the Xi’an Jiaotong Stomatological Hospital Affiliated to Xi’an Jiaotong University (No. 2025-XJKQIEC-XJS-0003-001). The patient gave written informed consent to publish all of the images, clinical data, and other data.
Author contributions: Xiang Liang and Chengpeng Lv performed the surgery. Linyang Xie and Sina Ahmadi managed the clinical care; patient management conducted the investigations, and data collection and analysis were carried out by Linyang Xie and Sina Ahmadi. Sina Ahmadi and Xiang Liang drafted and edited the manuscript. The project was supervised by Junbo Tu and Sijia Na. All authors reviewed and approved the final manuscript.
Funding: This work was supported by the Central University Basic Scientific Research Business Expenses Special Funds, China (Grant No. xzy012020048).
Consent for publication: This is a retrospective analysis, with the consent of the patients.
Data availability statement: All dates are included within the article. Videos of robot-assisted minimally invasive tooth extraction can be obtained upon reasonable request by contacting the first or corresponding author.
Conflicts of interest: The authors declare that there are no conflicts of interest financial, personal, or otherwise that could have appeared to influence the work reported in this manuscript. No author has any financial or non-financial relationship with any organizations that could inappropriately influence or bias the content of the paper.