Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Bolaji Paul
Msc (Healthcare Leadership), Consultant Stroke Physician and Education Lead, Dorset County Hospital, Dorchester, England.
Email: paul.bolaji@nhs.net
Received: Mar 03, 2026 Accepted: Mar 31, 2026 Published: Apr 07, 2026
Citation: Paul B, Emma H, Gagira M, Lawun T, Michelle D, et al. Erysipelothrix endocarditis acquired from household cat presenting with ischaemic stroke. Ann Case Rep Med Images. 2026; 3(1): 1078.
Copyright: Paul B et al. © All rights are reserved
A 75 yr old woman presented to our stroke service with acute onset of word finding difficulty and confusion. She was subsequently diagnosed with a left Middle Cerebral Artery (MCA) territory stroke. During admission she developed highgrade fevers and examination identified a diastolic murmur. Three sets of blood cultures were taken and consistently grew Erysipelothrix Rhusopathie. Transoesophageal Echocardiogram confirmed a mitral valve endocarditis. Erysipelothrix rhusiopathiae infection is rare and may result from exposure to cat faeces or scratches, as in this patient, who had contact with a cat. She subsequently had 6 weeks of intravenous antibiotics and was discharged home with package of care.
Erysipelothrix endocarditis is a very rare zoonotic infection with only a handful of cases in the literature. Whilst it is usually acquired from farm animals, especially fish and pigs, it is rarely associated with cats, a common household pet. Furthermore, Erysipelothrix endocarditis rarely presents as a stroke without preceding constitutional symptoms. This has epidemiological significance regarding the intertwined relationship of a communicable disease with a classical pathological disease such as stroke. This case hopes to shed more light on this unusual scenario.
The commonest aetiology implicated in cardioembolic stroke is atrial fibrillation [1]. However, it remains important to look for other cardiac causes of ischaemic stroke particularly in patients with atypical findings. Echocardiography is considered a routine investigation to identify structural or valvular heart disease or thrombus which may act as a focus for cardioembolic stroke. Infective endocarditis should be suspected in a patient who presents with fever, vasculitic and immunological phenomena or a new heart murmur on examination. Although native valve infective endocarditis is usually associated with streptococci, staphylococci and enterococci infection. Rare causes of endocarditis, including Coxiella, Erysipelothrix, and HACEK organisms, should also be considered [2].
Erysipelothrix rhusiopathiae is a gram-positive bacillus and zoonotic pathogen, most commonly affecting individuals who work with animals [3]. It commonly causes superficial skin infections but can progress to bacteraemia and endocarditis.
Human infections are rare and are due to exposure to infected animals, such as fish, swine, or other farm animals. Rarer sources are household pets like cats and dogs. There are three forms of human infection: localized erysipeloid, diffuse cutaneous form, and lastly, bacteraemia that could progress to Infective Endocarditis (IE) [4].
A 75-year-old woman was admitted with acute onset dysphasia and confusion. She had a background of hypertension, angina and chronic kidney disease. She lived alone with her cat and was otherwise fit and independent with all activities of daily living. Preceding constitutional symptoms and a history of cat bites could not be ascertained reliably because she lived alone and presented with confusion and language problems.
On initial examination, there were no peripheral stigmata of infective endocarditis. Cardiovascular examination revealed a grade 2/5 mid-diastolic murmur and a loud S1 at the mitral area, suggestive of mild mitral stenosis. She appeared disoriented and demonstrated both receptive and expressive dysphasia. Motor examination revealed normal power in all limbs, and there were no visual disturbances. A detailed assessment by the Speech and Language Therapist (SALT) identified poor attention, disorientation, perseveration, inability to follow twostage commands, and inconsistent reading performance.
CT imaging on admission demonstrated a sub-acute left temporoparietal infarct without haemorrhagic transformation, consistent with her presenting symptoms. Carotid Doppler and ECG findings were unremarkable. Initial blood tests showed elevated inflammatory markers, which were presumed to be reactive in the absence of clinical features of infection. By day five, the patient developed fever and confusion, accompanied by a further rise in inflammatory markers, prompting the collection of the first set of blood cultures. Empirical antibiotics were commenced for a presumed urinary tract infection.
Blood cultures subsequently grew Erysipelothrix rhusiopathiae after 11 hours of incubation, with a penicillin Minimal Inhibitory Concentration (MIC) of 0.023 mg/L. This was initially considered a potential contaminant; however, two additional sets of blood cultures obtained three days later again grew E. rhusiopathiae after 16 hours of incubation, confirming persistent bacteraemia. The microbiologist advised the need to exclude infective endocarditis, as persistent bacteraemia suggested a deep-seated infection.
A transthoracic echocardiogram revealed mild mitral stenosis, and subsequent transoesophageal echocardiography confirmed mitral valve endocarditis.
This patient did not undergo thrombolysis as she was a delayed presentation with a low National Institute of Health Stroke Severity score (NIHSS). She was subsequently started on high-dose aspirin and statins after a cranial CT scan excluded a haemorrhage.
Telemetry monitoring for 72 hours did not identify atrial fibrillation. Following confirmation of infective endocarditis, her case was discussed at the infective endocarditis Multidisciplinary Team (MDT), and it was agreed to treat with intravenous benzylpenicillin 1.2 g every 4 hours for six weeks, administered via a Peripherally Inserted Central Catheter (PICC) line.
A multidisciplinary rehabilitation program, including physical therapy, occupational therapy, and Speech and Language Therapy (SALT), was implemented to support recovery of her language impairment and restore functional abilities.
The patient showed clinical improvement with antibiotic therapy, as evidenced by a decline in inflammatory markers. Her agitation and disorientation largely resolved; however, her language impairment persisted. She developed new-onset anaemia, likely secondary to a combination of chronic kidney disease, infective endocarditis, and suspected diverticulosis. Iron supplementation was initiated, and a blood transfusion was administered once the infection had resolved. She was subsequently discharged home with a package of care.
One of the most common aetiologies for ischaemic strokes of cardioembolic origin, typically due to Atrial Fibrillation (AF) [1]. Sometimes this presentation may lead to the first recognition of AF in such patients. It is common practice to undertake secondary investigations to evaluate other causes of to exclude structural heart disease (such as left ventricular thrombus). Another cohort is young patients who present with stroke, as they do not usually have a history of ischaemic heart disease that could precipitate AF. We aim to complete inpatient echo in this group. Furthermore, we would consider bubble echo to identify atrial septal defects whereby venous emboli may reach the arterial circulation.
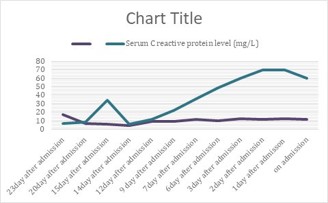
Figure 1: Trending inflammatory markers (i.e CRP and WBC).
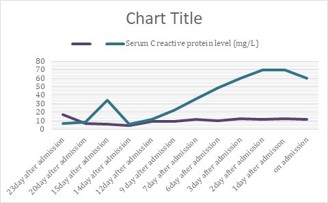
Figure 2: CT Brain at presentation demonstrating a subacute left temporoparietal infarcts.
Nonetheless, an important differential for the cardioembolic source is infective endocarditis leading to septic emboli in the brain, which can present insidiously. The diagnostic modality for this pathology is a Trans-Oesophageal Echocardiogram (TOE). Other atypical stroke features that suggest septic emboli include multifocal infarcts that affect both hemispheres. Furthermore, haemorrhagic transformation can be a common finding.
In a case report by Tan et al. [5] their patient presented with sudden onset blurred vision and a 3-day history of fever with an elevated ESR of 120 mm/hr. CT Head scan showed multi-focal infarcts with a microbleed. Urine dip was positive for erythrocytes (5+). Blood cultures and TOE were consistent with aortic valve endocarditis caused by Erysipelothrix rhusopathiae. In our index patient, her imaging demonstrated a left temporoparietal infarct. Urine dip was positive for blood and leucocytes. Treated initially as UTI. She later developed persistent fevers which prompted us to do a blood culture that grew Erysipelothrix rhusopathiae. TOE confirmed a native mitral valve endocarditis.
Stroke is a well-recognised complication of infective endocarditis. Neurological complications occur in 48-65% of the cardioembolic strokes. This typically involves an echocardiogram patient’s IE and this might often be the first presentation of the disease [5]. Septic emboli from infected vegetation can travel to the brain and other organs, potentially causing complications such as splenic infarcts.
The classical peripheral stigmata of IE are the immunologic and vasculitic phenomena. These are characterised by splinter haemorrhages, Osler’s nodes, Janeway lesions, Finger Clubbing, Roth spots in the fundus and myriads of other signs. These features, along with the blood cultures and echo findings form the diagnostic Duke’s criteria for IE [2].
The most common organisms that cause IE include Staphylococci, streptococci, and enterococci. Other less common organisms form the HACEK group (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella and Kingella species), Enterobacteriaceae, fungi, and Coxiella [2].
Although infections with E. rhusiopathiae are rare, endocarditis is a common complication, occurring in approximately 90% of reported cases.
It is however important to know that the bacteraemia can co-exist in patients without endocarditis as opined in the interesting case series of Challi et al. [6] titled “Erysipelothrix Bacteremia; is Endocarditis a Rule”. Other presentations of this bacteraemia could be septic arthritis, prosthetic joint infection, and osteomyelitis [7].
Erysipelothrix infection frequently causes extensive valve destruction and appears to have a greater affinity for the aortic or mitral valve [5,8]. The endocarditis may eventually lead to congestive heart failure, valve rupture and as seen in this case – cerebral infarction.
Erysipelothrix rhusiopathiae is an immobile, aerobic or facultatively anaerobic, non-sporing, non-motile, gram-positive bacillus. It is primarily a zoonotic pathogen [8]. Human infections are rare and are usually associated with occupational animal exposure, especially among fishermen, fish handlers, butchers, and veterinarians. Several wild and domestic animals, including fish and birds and rarely dogs, may shed the bacterium, but pigs are the most crucial reservoir [9]. In our index case, the patient lived alone with no contact with farm animals. The only plausible source of the infection was her pet cat. The household cat is a recognised zoonotic source of E. rhusiopathiae although only sparse literature exists about this association. The first case of erysipelothrix infection (without endocarditis), diagnosed after being bitten by stray cats, was published in 2019 [10].
In the absence of occupational exposures, risk factors for invasive E. rhusiopathiae infection are immunocompromised states, such as chronic kidney disease, diabetes mellitus, and treatment with high-dose steroids [11]. Major virulence factors in the pathogenesis are surface protective antigen, capsule polysaccharide gene (cpsA-C), rhusiopathiae surface protein (rspA and rspB), hyaluronidase (hylA-C), neuraminidase (nanH.1 and nanH.2), and adhesin [4].
E. rhusiopathiae infection can manifest in one of the following three forms: (i) a localized cutaneous lesion or erysipeloid, (ii) a generalized cutaneous form, and (iii) a septicaemia form, which is associated with infective endocarditis [4].
It is important to always look for any clues, especially on general examination in patient who present with strokes and fevers, to exclude infective endocarditis. That curiosity is sometimes important to make a diagnosis of IE early to ensure prompt treatment and prevent further septic embolic infarcts in the brain. If left untreated they can propagate into devastating haemorrhages and leave patients with significant morbidity and mortality.
Learning points/take home messages 3-5 bullet points
• In a patient with fever of unknown origin and recent stroke; It is important to examine the heart, undertake 3x sets of blood cultures and arrange an echocardiogram to exclude the possibility of infective endocarditis.
• This case represents a single non-haemorrhagic cerebral infarction as a presentation of Erysipelothrix rhusiopathiae IE. This is quite uncommon.
This is case of infection most likely originating from a household cat. Hence the need to be vigilant because cats, are common household pet for the zoonotic Erysipelothrix rhusopathiae infection.