Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Jun Wang
Department of Pathology and Laboratory Medicine, Loma Linda University Medical Center, Loma Linda, CA 92354, USA.
Email: JWang@llu.edu
Received: Feb 21, 2026 Accepted: Mar 09, 2026 Published: Mar 16, 2026
Citation: Borecky L, Leeper K, Wang J, Akhtari M. Co-occurrence of high-grade myeloid neoplasm and plasma cell myeloma-type post-transplant lymphoproliferative disorder. Ann Case Rep Med Images. 2026; 3(1): 1074.
Copyright: Wang J et al. © All rights are reserved
The co-occurrence of a myeloid and plasma cell neoplasm is an incompletely understood phenomenon with few cases reported in the literature. Even rarer is the coexistence of two separate hematologic malignancies in a post-transplant patient. We present a unique case of a concurrent acute myeloid neoplasm with monocytic differentiation and monomorphic plasma cell myeloma-type post-transplant lymphoproliferative disorder in a patient with a history of renal and pancreas transplant 12 years prior. This case illustrates diagnostic and therapeutic challenges, including the masking of malignant proliferating hematopoietic cells by cytopenia and cytological dysplasia, which are common side effects of immunosuppressant therapy, and the conflicting therapeutic strategies of reducing immunosuppression to treat acute myeloid leukemia and post-transplant lymphoproliferative disorder while balancing the increased risk of graft rejection.
Keywords: Acute myeloid leukemia; Post-transplant lymphoproliferative disorder; Monomorphic plasma cell myeloma-type post-transplant lymphoproliferative disorder; Plasmacytoma-like post-transplant lymphoproliferative disorder; Solid organ transplant.
Few cases in the literature describe the co-occurrence of a myeloid and plasma cell neoplasm. In some instances, treatment for a plasma cell dyscrasia such as multiple myeloma or Monoclonal Gammopathy of Undetermined Significance (MGUS) results in therapy-related myeloid neoplasm such as therapy-related myelodysplastic syndrome (MDS) [1-3]. This is thought to occur due to Deoxyribonucleic Acid (DNA) damage from cytotoxic chemotherapy agents that can damage the hematopoietic stem cells and lead to mutations that can transform into MDS, eventually progressing to Acute Myeloid Leukemia (AML) [4]. In other instances, a myeloid neoplasm such as Myelodysplastic Syndrome (MDS) or acute myeloid leukemia (AML) arises first, and a plasma cell proliferative disorder such as reactive plasmacytosis and rarely multiple myeloma can develop following induction chemotherapy [5]. Even rarer cases of de novo concurrent myeloid and plasma cell neoplasms without prior chemotherapy have also been reported [6-8]. Although the risk for developing a hematologic malignancy increases with age, solid organ transplant patients are at additional risk of developing malignancies, especially carcinomas, due to long- term immunosuppression [9,10]. The incidence of developing leukemia in solid-organ transplant patients is approximated to be five times higher than the general population [10]. Despite this, only a few published cases describe the development of an acute myeloid leukemia following solid organ transplant [10,11]. Further, although lymphoproliferative disorders, especially B-cell neoplasms associated with Ebstein-Barr Virus (EBV), have been reported in solid-organ transplant patients, very rarely do the lymphoproliferative disorders show monoclonal plasma cell differentiation [12-15]. We present a unique case of a simultaneous acute myeloid neoplasm with monocytic differentiation and monomorphic plasma cell myeloma-type Post-Transplant Lymphoproliferative Disorder (PTLD) in a patient with a history of renal and pancreas transplant 12 years prior.
A 48-year-old male with history of chronic obstructive pulmonary disease, previous tobacco usage (quit 13 years ago), uncontrolled type 1 diabetes, chronic kidney disease stage 3b secondary to diabetes status post renal and pancreas transplant 12 years prior, current immunosuppression (on Tacrolimus, Mycophenolic acid, and Prednisone), and chronic anemia was sent to an emergency department at an outside hospital after routine pre-nephrology labs showed severe pancytopenia. Upon presentation, the patient complained of easy bruising on the arms, fatigue, exertional dyspnea when using the stairs, chills/cold sensation, and one day of relatively lower glucose readings. The patient denied fever, gum bleeding, hematuria, melena, hematochezia, and chest pain. Family history was significant for hypertension and diabetes with no known hematologic malignancies or bone marrow disorders.
Vitals on admission were unremarkable (blood pressure 122/81; heart rate 96 beats per minute; peripheral oxygen saturation 99% on room air). Physical exam was significant for ecchymoses over bilateral forearms with no diffuse petechiae or rashes and a mildly fatigued appearance.
The Complete Blood Count (CBC) with differential re- demonstrated pancytopenia with severe neutropenia (Table 1), prompting an urgent hematology consult to evaluate for drug-induced marrow suppression, viral etiologies such as Cytomegalovirus, aplastic anemia, PTLD, or calcineurin-inhibitor- associated thrombotic microangiopathy with hemolysis. Further work-up showed a detectable hepatitis C virus antibody without current active infection. The patient was started on broad- spectrum intravenous antibiotics per neutropenic protocol, and a bone marrow biopsy was done.
| Reference range and units | Values |
|---|---|
| WBC 4.4-10.8*103/uL | 0.9 (Low) |
| RBC 4.5-5.90*106/uL | 2.65 (Low) |
| Hgb 13.5-17.5 g/dL | 7.7 (Low) |
| Hct 41.0-53.0 % | 24.0% (Low) |
| MCV 80.0-100.0 fL | 90.7 |
| MCH 28.0-32.0 pg | 29 |
| MCHC 32.0-36.0 g/dL | 32 |
| RDW 11.8-14.3% | 20.3 (High) |
| Plts 140-450 X 103/uL | 11 (Low) |
| MPV 6.9-10.8 fL | 9.9 |
| Neutrophils % (Manual) 37.0-80.0 | 15 (Low) |
| Monocytes % (Manual) 0-12 | 13 (High) |
| Eosinophils % (Manual) 0-7 | 3 |
| Basophils % (Manual) 0-2 | 0 |
| Platelet estimate | Markedly decreased |
| Anisocytosis (Manual) | Slight |
| Microcytosis | Slight |
| Macrocytosis | Slight |
| Reticulocyte Count (auto) 0.5-1.5% | 1.05 |
| Hemoglobin A1C <5.7% | 9.2 (High) |
The outside bone marrow biopsy revealed acute myeloid leukemia with CD34 positive blasts comprising 30-40% of marrow cellularity. The biopsy also showed marrow involvement by a plasma cell neoplasm comprising 10% of marrow cellularity. C-kit immunostain highlighted abnormal kappa-restricted plasma cells. Outside flow cytometry of the bone marrow aspirate showed increased abnormal myeloid blasts (~26.7% of sample), relatively increased monocytic cells (~31% of sample), an abnormal monotypic plasma cell population (~0.3% of sample), and relatively increased population of T-cell large granular lymphocytes (~9.5% of sample). AML Fluorescence in Situ Hybridization (FISH) showed no assay specific abnormalities while Multiple Myeloma FISH detected a gain of chromosomes 7, 9, and 15. Three copies of the gene TP53 were detected in 35% of nuclei, indicating an abnormality in chromosome 17. An extra copy of the gene FGFR3 was observed in 28% of cells, indicating a chromosome 4 abnormality. An extra copy of the gene CCND1 in 35% of cells was also seen, indicating a chromosome 11 abnormality, most likely trisomy. No RUNX1T1/ RUNX1, FGFR3/IGH, or CCND1/IGH translocations were detected. Since the outside hospital did not provide oncology services, the patient was transferred for further evaluation and to establish care with our oncology. Upon admission, baseline labs were ordered, which redemonstrated pancytopenia as well as antibodies to Hepatitis C virus and Parvovirus B19.
A repeat bone marrow biopsy was performed, which confirmed a high-grade myeloid neoplasm consistent with AML with monocytic differentiation, presumed to evolve from a preexisting undiagnosed Myelodysplastic Syndrome (MDS), as well as 7-10% kappa-restricted plasma cells consistent with monomorphic plasma cell myeloma-type PTLD (Figure 1).
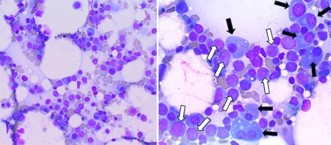
Figure 1: (Left) Wright-Giemsa stain of the repeat bone marrow aspirate smear at low power (40x,) showing scattered hematopoietic cells. (Right) Higher power view (400x) of the bone marrow aspirate smear highlighting an increase in both plasma cells (black arrows) and myeloblasts (white arrows).
The Hematoxylin and Eosin (H&E) stained bone marrow core biopsy section was hypocellular (~20-30% cellularity) with active trilineage hematopoiesis (Figure 2). Immunohistochemical staining of the decalcified trephine core biopsy sections showed an increase in immature myeloid precursors and plasma cells (Figure 2).
Kappa and lambda immunostains were performed to evaluate for a monoclonal plasma cell population, which was confirmed to be kappa light-chain restricted (Figure 3).
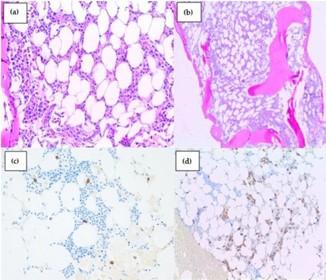
Figure 2: (A) Hematoxylin and eosin (H&E) stained bone marrow core biopsy section at high power (400x) and (B) low power (40x), highlighting a hypocellular marrow (20-30%) with scattered hematopoietic cells (purple dots), marrow fat (white clear circles), and marrow bone trabeculae and spicules (pink solid components). (C) High power (400x) view of the CD117 immunostain, which highlights an increase in immature myeloid precursors (brown circles). (D) Low power view (40x) of the CD138 imunostain, which shows an increase in plasma cells (brown circles).
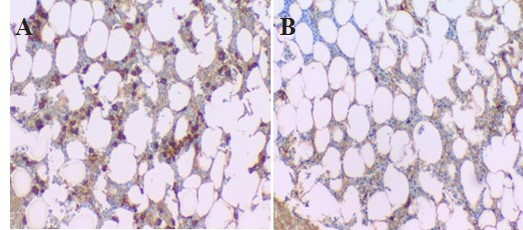
Figure 3: (A) High power view (400x) of kappa light chain immunostain, showing an increase in kappa light chain restricted plasma cells (brown circles). (B) In comparison, note the near absence of lambda light chain staining in these plasma cells (400x).
Chromosome analysis was abnormal, showing terminal deletion of the long arm of chromosome 20 (20q). The AML FISH panel for the repeat bone marrow biopsy showed trisomy of chromosome 5 and deletion of the long arm of chromosome 20 (20q). The Multiple Myeloma FISH panel was also abnormal, showing trisomy of chromosomes 2, 3, 6, 7, 11, and 17, and one less copy of the MAFB gene, suggesting a deletion involving 20q. Next Generation Sequencing for myeloid neoplasms showed pathogenic mutations in CSF3R (5%), DNMT3A (4%), RUNX1 (44%), WT1 (5%), and ZRSR2 (49%). Altogether, the FISH results were consistent with a hyperdiploid karyotype.
Treatment
In consideration of the patient’s pre-existing renal dysfunction, cycle 1 Decitabine/Cedazuridine was started with transfusion support (3 units of packed red blood cells (pRBCs) and 3 platelet units). For the plasma cell myeloma-type PTLD, the patient was started on outpatient bortezomib (Velcade) with dexamethasone weekly. The patient remained profoundly neutropenic and was maintained on antimicrobial prophylaxis Acyclovir and Levaquin with neutropenic precautions.
Endocrinology managed the patient’s labile type 1 diabetes mellitus with transition to scheduled basal/bolus insulin after episodes of hypoglycemia followed by marked hyperglycemia. Transplant nephrology managed the acute kidney injury in the setting of chronic kidney disease in the kidney allograft with fluids and adjustment of tacrolimus, resulting in down-trending creatinine. Renal allograft ultrasound showed mildly elevated intrarenal RI (resistance index) without stenosis. The patient was discharged after being deemed hemodynamically and medically stable.
At the first follow-up outpatient hematology oncology appointment, a repeat CBC showed severe leukopenia, severe neutropenia, severe normocytic anemia, and severe thrombocytopenia with no need for additional transfusions. The Comprehensive Metabolic Panel (CMP) showed elevated blood urea nitrogen and creatine, consistent with the patient’s renal dysfunction. For AML, the patient was started on Inqouvi in combination with Venetoclax. For the plasma cell myeloma- type PTLD, the weekly Velcade injections and Dexamethasone were continued. For antimicrobial prophylaxis, Cresemba antifungal was added in addition to the daily Acyclovir and Levaquin. Famotidine was also started at this time to treat medication side effects.
At subsequent outpatient hematology oncology appointments, the patient has continued ongoing treatment as described above with persistent fatigue, shortness of breath, and bruising along with recent chest pain/tightness, cough with phlegm, low grade fever, chills, and tachycardia.
Labs have re-demonstrated abnormal renal function and severe pancytopenia requiring pRBC and platelet transfusions as needed. Notable events include a brief admission at an outside hospital for shortness of breath and bilateral leg swelling where the patient was found to have neutropenic sepsis due to pneumonia and a urinary tract infection with cultures positive for E. coli and micrococcus species, treated with Vancomycin. At the time this case report was written, the patient continues to receive ongoing treatment as described above.
This case illustrates the importance of considering malignancy, particularly the possibility of a hematologic malignancy and/ or multiple uncommon entities occurring simultaneously, in a post-transplant patient. As solid organ transplant patients must undergo long-term immunosuppression to prevent acute rejection, their risk for developing a malignant tumor such as lymphoproliferative disorder, Kaposi sarcoma, or skin cancer increases 2 to 4-fold when compared with the general population [16]. This is because the host immune system is weakened by long term immunosuppressants, leading to reduced detection of pro-oncogenic cells and activation of oncogenic viruses [16].
The diagnosis of hematologic malignancies in post-transplant patients can be challenging due to the masking of symptoms and lab findings by common side effects of immunosuppressant drugs. For instance, the diagnosis of AML in a post-transplant recipient is often misled by cytopenia, infections, and cytological atypia, all of which are common findings after transplantation [10]. The diagnosis of a monomorphic plasma cell-type PTLD can also be challenging due to the commonality of finding plasma cell rich infiltrates in acute rejection, and plasmacytic hyperplasia and plasma cell rich polymorphic lymphoproliferations in early PTLD lesions [15].
However, these plasma cell infiltrates are usually a mixed population with no light chain restriction or clonal population identified, unlike the kappa-restricted monomorphic plasma cells detected in our patient’s bone marrow specimen [15].
The coexistence of multiple hematologic malignancies in a post-transplant patient also presents many therapeutic challenges. For instance, the initial therapy for PTLD and AML is a reduction of immunosuppression, which increases the risk of graft rejection or loss [15]. In some cases, targeted chemotherapy after reduced immunosuppression with agents such as myelotoxic Azacitadine or proteasome-inhibitor based regimens for plasmacytoma-like PTLD resulted in improved survival and remission overall when paired with stem cell transplantation in post-transplant patients with AML or plasmacytoma-like PTLD respectively [10,11,14]. However, some cases of co-occurring MDS and MGUS/Multiple Myeloma showed chemoresistance, with some studies suggesting more aggressive treatment and earlier stem cell transplantation to improve overall survival [1]. Further investigation of the risks and most effective treatment strategies for concurrent myeloid and plasma cell neoplasms in post-transplant patients could contribute to improved outcomes for this unique patient population.
This case also presents a unique picture of multiple uncommon entities occurring simultaneously. For instance, most PTLDs are associated with EBV infection and are B-cell lymphomas, with Diffuse Large B Cell Lymphoma (DLBCL) being the most common entity and the digestive system as the most common extranodal site [17]. In our case, EBV was negative with a monomorphic plasma cell myeloma-type PTLD, which only comprises 3.5% of PTLD subtypes, presents 3-10 years (median time) after transplant, and is usually characterized by CD138 expression with a lack of CD20 and no significant symptoms commonly associated with multiple myeloma such as bone lesions or hypercalcemia [14]. Further, this case adds another example of a coexisting myeloid and plasma cell neoplasm to the existing literature. Although the mechanism of a concurrent myeloid and plasma cell malignancy is incompletely understood, the separate entities likely arise from two separate clones as whole genome sequencing for 27 patients with co-occurring MDS and multiple myeloma, MGUS, or plasmacytoma found no common founder mutation [1]. In cases of AML with plasmacytosis, some theorize that the production of interleukin-6 by leukemic blasts can lead to excessive plasma cell proliferation [5]. As many documented cases of hematologic malignancies in post-transplant patients seem to occur in renal transplant patients, future studies could investigate whether there is an increased risk of developing hematologic malignancies in kidney transplant patients when compared to other solid organ transplant patients.
In conclusion, simultaneous AML and monomorphic plasma cell myeloma-type post-transplant lymphoproliferative disorder in a post-transplant patient is a rare, serious complication that arises from long-term immunosuppression and requires complex management involving immunosuppression reduction, chemotherapy, targeted agents, and stem cell transplantation. It provides therapeutic challenges because treatments for the hematologic malignancies may increase the risk of graft rejection or loss, necessitating tailored strategies focusing on both the malignant plasma cells and AML clone while maintaining adequate immunosuppression to ensure graf t survival.
Author contributions: Conceptualization, J.W., M.A., and L.B.; writing—original draft preparation, L.B..; writing—review and editing, L.B., K.L., J.W.; visualization, L.B., K.L., J.W., M.A.; supervision, J.W., M.A. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional review board statement: The Loma Linda University Institutional Review Board does not consider a single-patient case report to be research and accordingly does not require ethical approval.
Informed consent statement: The patient provided oral informed consent for publication of this case and any necessary accompanying images.
Conflicts of interest: The authors declare no conflicts of interest.
Abbreviations: MGUS: Monoclonal Gammopathy of Undetermined Significance; MDS: Myelodysplastic Syndrome; DNA: Deoxyribonucleic Acid; AML: Acute Myeloid Leukemia; CBC: Complete Blood Count; PTLD: Post-Transplant Lymphoproliferative Disorder; WBC: White Blood Cells; RBC: Red Blood Cells; Hgb: Hemoglobin; Hct: Hematocrit; MCV: Mean Corpuscular Volume; MCH: Mean Corpuscular Hemoglobin; MCHC: Mean Corpuscular Hemoglobin Concentration; RDW: Red Cell Distribution Width; Plts: Platelets; MPV: Mean Platelet Volume; dL: Deciliter; uL: Microliter; fL: Femtoliter; pg: Picograms; FISH: Fluorescence in-situ Hybridization; pRBC: Packed Red Blood Cells; CMP: Comprehensive Metabolic Panel; RI: Resistance Index