Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Boukettaya Wiem
Department of Medical Oncology, Farhat Hached Hospital Sousse, Faculty of Medicine of Sousse, Tunisia.
Email: wiemboukettaya@gmail.com
Received: Feb 17, 2026 Accepted: Mar 04, 2026 Published: Mar 11, 2026
Citation: Wiem B, Khawla K, Emna N, Mariem B, Abdelkader M, et al. A rare case of a pediatric low grade appendiceal mucinous neoplasms and review of literature. Ann Case Rep Med Images. 2026; 3(1): 1073.
Copyright: Boukettaya W et al. © All rights are reserved
Colorectal cancer is extremely rare in children. Primary appendiceal carcinomas are often found incidentally when the appendix is surgically removed. Appendiceal Mucinous Adenocarcinomas are even less common. We report a case of a 10-year-old girl presented with abdominal pain associated with vomiting episodes. Abdominal ultrasound and biopsy confirmed a Low Grade Appendiceal Mucinous Neoplasms (LAMN). The aim of this report is to shed light on the management and surveillance of LAMN after resection, especially in a pediatric patient.
Keywords: Appendiceal neoplasm; Pediatric; Mucine; Low grade appendiceal mucinous carcinoma.
Primary Appendiceal neoplasms are a rare pathological finding, present in >2% of appendicectomies [1]. In Pediatric population it represents less than 1% of all neoplasms in the first two decades of life [1,2]. They are commonly diagnosed after surgical intervention for acute Appendicitis or assumed Ovarian malignancy [2], whilst specifically Appendiceal Mucinous Adenocarcinomas are even less common; presenting in 0.2% of Appendicectomies [1]. Histologically, these neoplasms can be divided into Low Grade Appendiceal Mucinous Neoplasms (LAMN) and High-Grade Mucinous Neoplasms (HAMN); both non-invasive [3]. In this report, we describe a case of a Low Grade Appendiceal Mucinous Neoplasms in a 10-year-old-girl.
A 10-year-old-girl presented with abdominal pain associated with vomiting episodes and dizziness. Abdominal ultrasound showed a swollen laterocaecal appendix of about 10 millimeters at the greatest diameter with histosonographic dedifferentiation of its parietal tunics and hyperechoic infiltration of the peri-appendicular fat (Figure 1A & 1B).
The diagnosis of acute Appendicitis was established and the patient underwent surgery. A retrograde appendicectomy was performed. During the procedure, the appendix was gangrenous and no intra-peritoneal mucin or intra--peritoneal malignant disease was seen. Specimen pathology revealed a low grade Appendiceal mucinous neoplasm LAMN into the appendiceal wall with healthy margins (Figure 2A, 2B & 2C).

Figure 1A: Longitudinal ultrasound view of the appendix demonstrating a diameter of 0.91 cm.

Figure 1B: Transverse ultrasound view of the appendix demonstrating a diameter of 0.73 cm.
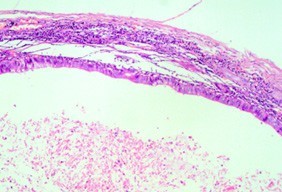
Figure 2A: HE staining showing cystic dilatation of the appendiceal wall.
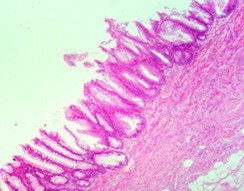
Figure 2B: HE staining showing dyspastic epithelium at medium magnification.
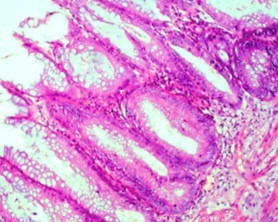
Figure 2C: HE staining showing dyspastic epithelium at medium magnification.
Colonoscopic evaluation was normal. A postoperative Computed Tomography (CT) was performed on the chest abdomen and pelvic showed a suspicious densification of omental fat with left mediastinal and supraclavicular adenomegaly. The case was presented in a multidisciplinary reunion and a radiologic with biologic follow up was indicated.
Mucinous neoplasia of the appendix is a rare condition that occurs in approximately 1% of the patients undergoing appendectomy [4].
Reports on cases of Mucinous Adenocarcinomas remain few. Appendiceal mucinous neoplasms are seldom seen in the pediatric population with an incidence of one in one million [5,6], as they typically present in the sixth decade of life
A common theme in the literature describing such cases is that initial presentation may mimic acute Appendicitis symptoms such as pain in the right iliac fossa, fever, nausea, and vomiting like our patient.
Alemayehu et al. reported the incidence of unexpected pathology findings after appendectomy in 3602 children over a 16- year period, and none were found to have a mucinous neoplasm [7].
Pai et al. found only two patients under 20 years over 116 cases of appendiceal mucinous neoplasms in 30 years follow-up [8].
LAMN are typically defined as lesions confined to the appendix without evidence of invasion or disseminated peritoneal disease [9].
LAMN with acellular mucin in the right lower quadrant showed a lower risk (4-8%) of recurrence or progression to pseudomyxoma peritonei (PMP), contrarily to LAMN with cellular mucin that demonstrates a higher risk of disseminated disease (33–75%) [10].
Best management strategies, as well as time to treatment, are unclear because of the rarity of LAMN [11]. Surgical resection is the recommended treatment for LAMN. When LAMN is confined to the appendix, complete resection by appendectomy with a negative proximal margin is sufficient for cure [12]. Our patient had an appendectomy with negative margin.
In cases with extra-appendiceal spread, complete resection of the appendix is necessary along with resection of any grossly involved surrounding peri-appendiceal tissue or implants. Right hemicolectomy is only indicated for invasive adenocarcinomas without peritoneal disease [13]. Cytoreductive surgery with intraperitoneal chemotherapy is recommended for disseminated peritoneal disease.
Pathologic examination of our patient’s specimen verified a LAMN confined to the mucosa and a negative cecal margin, corroborating complete resection and cure.
There is no standard recommendation for surveillance of LAMN after resection, especially in a pediatric patient who would necessitate long-term observation.
Guaglio M and al [14] promote for LAMN with or without limited peritoneal spread a follow-up assessment included thoracic-abdomino-pelvic computed tomography scan and serum tumor markers scheduled after surgery, then every 6 months for 5 years, and yearly thereafter. Similar to him in patients with low-risk LAMN, McDonald et al. [15] recommended a watch-and-wait policy with surveillance imaging at 6 months, then annually. For ruptured neoplasms, Murphy et al. [16] recommends baseline tumor markers and a CT scans every year for 5 years, then every 2 years for 10 years to monitor for any long-term recurrence
Although Appendiceal mucinous neoplasms are is an exceedingly uncommon pathology tumor in the pediatric population they should be considered when a mucocele is identified pre-operatively or intra-operatively. It is a low-grade neoplasm treated by complete surgical resection when confined to the appendix.
Further studies are needed to assess the long-term surveillance and follow-up specially for pediatric patients with LAMN.