Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Boryana Avramova
Department of Pediatric Hematology and Oncology, University Hospital “Queen Joanna–ISUL,” Sofia, Bulgaria.
Email: b.avramova@isul.eu
Received: Feb 09, 2026 Accepted: Feb 26, 2026 Published: Mar 05, 2026
Citation: Boronsuzov I, Shtarbanov I, Avramova B. Two cases of pediatric colorectal carcinoma with atypical presentation. Ann Case Rep Med Images. 2026; 3(1): 1071.
Copyright: Avramova B et al. © All rights are reserved
Keywords: Colorectal carcinoma; Children; Atypical presentation; Malignancy; Computed tomography.
Pediatric colorectal carcinomas are very rare cancers, particularly before puberty, with annual incidence of 1-2/1,000,000 cases [1,2]. From all cases only 1-4 % occurs in children and adolescents [2]. In pediatric group the tumor is more frequent in male aged above 15 years [3].
Very often the disease presented with advanced stages and has distinct histological and molecular characteristic. In most of the cases the presenting symptoms are nonspecific [4]. Because of their rarity and nonspecific course, early diagnosis and successful treatment remain a challenge [3].
Risk factors for colorectal carcinoma in children are the same as in adults with greater influence of hereditary syndromes, but poor prognostic factors are more common in children [2]. The most important prognostic factors in these patients are histological type and stage of the disease.
In this report we describe two cases of children with colorectal carcinoma with unusual clinical presentation and many difficulties in the diagnosis. In the first case the malignant disease was presented in a metastatic stage with an unclear primary localization. In the second the initial clinical presentation is spleen abscess, which delay the diagnosis.
A 17 years old girl presented with fever, weight loss, and intermittent abdominal and diffuse bone pain was admitted in the pediatric surgery department. She had no family history of malignancy and hereditary syndromes, and did not have any chronic diseases in the past. During the physical examination diffuse abdominal pain and an asymmetry of the breasts were observed (the right breast was larger than left with thickened skin around the areola). No other abnormalities in other organs or systems were found. The all-vital signs were normal.
The physicians in surgical department were performed some diagnostic tests, including ultrasound and Computer Tomography (CT) scan. Hepatomegaly with multiple diffuse hepatic metastases, multiple diffuse pulmonary metastases, and a solitary bone metastasis in the 4th lumbar vertebra was visualized in the whole-body CT scan. No primary localization of the malignancy has been established.
A biopsy of liver metastasis was recommended, but the parent's refusal has been declared. A working diagnosis was metastatic carcinoma, with suspected primary localization in the right breast. The child was transferred to our department for further diagnosis and treatment.
On admission in the pediatric oncological department, the patient was in poor general condition, with a marked reduction of subcutaneous adipose tissue and massive hepatomegaly reaching umbilical horizontal. Tumor marker analysis revealed significantly elevated Carcinoembryonic Antigen (CEA) (2,100 ng/ml; normal range – 0-5 ng/ml) and Cancer Antigen (CA) 19-9 levels (14,700 U/ml; normal range – 0-37 U/ml). A whole-body CT scan was re-conducted. Mammography and ultrasound of the breasts and abdomen were done but the primary tumor localization has not been identified. As a next diagnostic step, Positron Emission Tomography (PET/CT) was performed, with result of significant metabolic activity in proximal rectum (primary localization) (Figure 1A), with the previously identified multiple liver (Figure 1B) and lung metastases (Figure 1C). In addition to the metastasis of the 4th lumbar vertebra, we were found multiple bone metastases of the axial skeleton, pelvic bones bilaterally, and in the head of the left humerus (Figure 1D). A colonoscopy was performed, which revealed a large tumor formation in the proximal part of the rectum with stenosis of the lumen. Biopsy was taken. The result of the histological examination is well differentiated colorectal adenocarcinoma. The final diagnosis was colorectal cancer with metastases in the liver, lung and bones. After diagnosis and staging of the disease, treatment was continued at another hospital abroad and we lost the patient of follow-up.
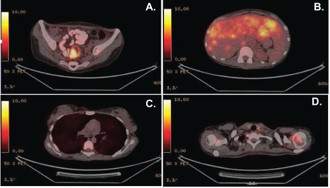
Figure 1: PET/CT scan images for Case #1. (A) PET/CT image of the primary tumor with localization in the proximal rectum. (B) PET/CT scan image of massive liver involvement from underlying disease. (C) PET/CT image of diffuse bilateral pulmonary metastases. (D) PET/CT imaging of bone metastasis in the head of the left humerus.
A 17 years old boy was admitted in the department of pediatrics due to a gastric pain and fever. The patient had no family history of malignances or past history of hereditary syndromes. An abdominal ultrasound was performed and spleen formation was found. The diagnosis of a spleen abscess was accepted. All inflammatory markers (white blood cells count, erythrocyte sedimentation rate and C-reactive protein) were elevated (WBC – 15.3 G/l, normal range – 3.5-10.5 G/l; ESR-120 mm/h, normal range – up to 20 mm/h; CRP-8.2 mg/dl, normal range – 0-0.6 mg/dl). No other signs or symptoms were found. Vital signs were normal.
Antibiotic treatment was started, but due to worsening of the general condition and not improvement of the described symptoms, he was transferred urgently to the pediatric surgery department where a laparotomy was performed. Intraoperative, two abscesses of the spleen were found, with penetration from the colon descensus to the spleen. Extensive resection of the affected colon area with splenectomy was performed. The result of the histological examination was low differentiated mucinous colorectal carcinoma.
Postoperative, a staging whole-body CT scan were performed, from which a solitary, 17 mm metastasis was detected in the 8th segment of the liver. The levels of tumor markers CEA and CA-19-9 were normal (CEA-2.47 ng/ml; CA-19-9-6.3 U/ml). The final diagnosis was colorectal carcinoma with liver metastasis (stage IV).
In pediatric oncological department six courses of FOLFIRI chemotherapy (calcium folinate 400 mg/m2 on day 1, 5-fluorouracil – 400 mg/m2 bolus on day 1 and 2500 mg/m2 more than 46 hours continuous infusion, irinotecan – 180 mg/m2 on day 1) every 14 days were performed, with very good result complete treatment response of the primary disease. The therapy was continued with six more courses.
Three months after the end of therapy, a local relapse (in the upper part of the colon) of the disease was diagnosed, and the second line treatment continued at the adult oncological department (we have no exact information). Despite the therapy, the patient died 6 months after the diagnosis of relapse due to progression of the disease.
Colorectal carcinoma is an extremely rare disease in childhood. In the United States, about 80 cases are diagnosed annually in patients under the age of 20, which correspond to a frequency of about 1-2/1,000,000 [1,4,5]. The incidence is different in every country. Australia, New Zealand, Europe, and North America are estimated to have the highest incidence rates, whereas Africa and South-Central Asia have the lowest rate [4,6]. Characterized by its biological and clinical features, the main distinguishing characteristics are the prevalence of the unfavorable mucinous histologic type and very oft diagnosis in advanced stages, which also predetermines the less favorable final prognosis [7,8].
In the largest described series of 77 colorectal carcinoma patients between the ages of 7 and 19 treated for the period 1964-2003 at St. Jude Hospital, 62% were the relative proportion of mucinous histologic variants. Eighty six percent of the patients were diagnosed at an advanced stage, and more than half had metastases at diagnosis. The 10-year survival rate was 17% [9]. Although in the before mentioned series, the youngest patient was 7 years old, in the literature the youngest patient described was 9 months old [10].
As in adults, sporadic cases predominate, with less common predisposing factors such as hereditary syndromes ((familial adenomatous polyposis, Lynch syndrome and juvenile polyposis) with increased frequency of colorectal carcinoma [2].
The clinical characteristics are similar to those in adults – abdominal pain, gastrointestinal bleeding, anemia, changes in defecation. Due to the rarity of the disease and the nonspecific syndromes, the frequently described manifestations can be attributed to other diseases [11].
In our two cases some rare and unusual for colorectal cancer presentation were observed. Patient No. 2 was initially diagnosed with an abscess of the spleen before the final diagnosis of colorectal cancer was made. According to the literature, the incidence of perforation in colon cancer is about 2%-10%, with abscess formation only in 0.3%-4% [12].
For patient No. 1 general constitutional manifestations and bone pain dominated as clinical symptoms. Bone metastases are rare in colorectal cancer, especially in pediatric patients. Their frequency is about 1% [13]. Their most common localization is in the spine. The presentation of bone metastatic disease is the cause of a misdiagnosed breast cancer at the first hospitalization.
The main imaging techniques for diagnosing and staging of the colorectal cancers are colonoscopy or CT colonography for visualization of the primary tumor. Contrast X-ray colonography and intestinal ultrasonography have low sensitivity and cannot be used to rule out the disease. The staging is done mainly by CT scan on the chest and abdomen. PET/CT scan is not approved as the initial imaging method in colon cancer. Mucinous carcinoma, which prevails in childhood, is characterized by even a reduced accumulation of radioisotope, which further limits the use of the method [13]. In our patient No. 1 who had classical colon cancer, the PET/CT was the method, which most accurately visualized the primary tumor and the metastatic localizations (Figure 1), especially the bone metastases. The CEA tumor marker is of limited value for the follow-up of pediatric patients with verified diagnosis of colorectal cancer [10].
Given the rarity of the disease, no large randomized trials of the treatment of colorectal carcinoma in children have been conducted. The recommendations in adults are surgery of the primary tumor and metastases for oligometastatic disease. Adjuvant chemotherapy is applied in stage III and in selected patients in stage II. Palliative chemotherapy and targeted therapy with Bevacizumab (Avastin) are the main methods for treating patients with metastatic disease, including children [12,14]. This type of therapy was not effective in our patient and he died from the disease progression one year after the diagnosis.
Colorectal carcinoma occurs in childhood rare and presented in most cases in advanced stages. Due to this reason the diagnosis of malignant colorectal tumor should be taken into account in all patients with unspecified gastrointestinal symptoms. Early diagnosis with imagine technics and promptly treatment are the major factors which improve the prognosis of the disease.
Clinical practice points
• Colorectal carcinoma is rare in children and is characterized by an aggressive course, nonspecific clinical presentation, and unfavorable prognosis. Early diagnosis is crucial for successful treatment.
• Early diagnosis using imaging techniques and prompt treatment are the major factors that improve the prognosis of the disease.
• Due to its rarity in children, physicians should consider carcinoma in all cases of nonspecific gastrointestinal symptoms and suspected malignancy.
Acknowledgments: We would like to thank the staff of the Nuclear Medicine Department and PET/CT Center at “Alexandrovska Hospital” for the imaging studies. Also, to Dr. Ventsislav Nakov† from the Department of Gastroenterology in the University Hospital “Queen Joanna” for endoscopy and biopsy of the tumor formation in case 1.
Consent form: At the admission in the hospital the parents of the patients signed inform consent.
Conflict of interest: All authors declare no conflict of interest.
Author’s contribution: All authors have equal contribution in the work. B. Avramova is corresponding author.
Funding: This work didn't receive grants from any funding agency in the public, commercial or not-for-profit sectors.