Article Type: Research Article, Volume 3 Issue 1
*Corresponding author: Fen Wang
Department of Radiation Oncology, University of Kansas
Medical Center, USA.
Email: fwang1@kumc.edu
Received: Feb 01, 2026 Accepted: Feb 24, 2026 Published: Mar 03, 2026
Citation: Gadam RK, Wang F. Radiation therapy for pseudotumor of skull base: A single institutional case series. Ann Case Rep Med Images. 2026; 3(1): 1070.
Copyright: Wang F et al. © All rights are reserved
Background: IgG4-related skull base pseudotumor is a benign fibroinflammatory disorder involving tissues of the skull base. If inadequately controlled, it may progress to a more diffuse disease with involvement of the optic nerve, additional cranial nerves, and skull bones. Histopathology typically demonstrates lymphoplasmacytic infiltrates with abundant IgG4-positive plasma cells. First-line treatment consists of corticosteroids and immunosuppressive therapy; however, refractory cases may require surgical intervention or radiation therapy. We report two cases of IgG4-related pseudotumor treated with radiation therapy, achieving good clinical response with minimal toxicity.
Case presentations: A 56-year-old woman with IgG4-related pseudotumor of the skull base underwent two emergent left mastoidectomy procedures and experienced continued disease progression despite corticosteroid therapy, with multiple recurrences. She was treated with intensity modulated radiation therapy (IMRT) to a total dose of 4000 cGy in 20 fractions. At 76 months of follow-up, her symptoms and radiographic findings demonstrated near-complete resolution.
A 69-year-old man with multiple medical comorbidities was diagnosed with IgG4-related pseudotumor and showed disease progression despite multiple courses of corticosteroids and rituximab, ultimately developing multiple cranial nerve neuropathies. He was treated with IMRT to a total dose of 3000 cGy in 15 fractions. His symptoms remained stable at 6 months of follow-up.
Conclusion: In patients with IgG4-related skull pseudotumor presenting with diffuse disease and severe symptoms refractory to medical or surgical management, short-course radiation therapy using IMRT with daily Image-Guided Radiation Therapy (IGRT) can provide effective local control, symptom relief, and minimal toxicity.
Keywords: Skull base pseudotumor; IgG4-related disease; Radiation therapy; Idiopathic orbital inflammatory syndrome.
Pseudotumor of the skull base is a benign but potentially aggressive fibroinflammatory disease with the capacity for local invasion and significant morbidity, including vision loss, hearing loss, and severe persistent pain. It is variably referred to as Immunoglobulin G4 (IgG4)–related skull base pseudotumor. Although etiology remains unclear, an autoimmune mechanism has been strongly hypothesized [1,2].
This disease may involve tissues surrounding the skull base, including orbit, mastoid bone, and cranial nerves. If left uncontrolled, it may progress to diffuse involvement, including optic nerve compression resulting in vision loss and skull base or mastoid bone involvement leading to hearing impairment [3,4].
Clinical presentation is variable but commonly includes acute orbital pain, diplopia, visual disturbances, eyelid swelling, restricted ocular motility, chemosis, and erythema of the eyelids and sclera [5]. Patients often present later in the disease course, and diagnostic evaluation is primarily directed toward excluding infectious and malignant etiologies.
Imaging plays a central role in diagnosis and includes Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) of the orbit and skull base. Typical radiographic features include homogeneous contrast enhancement and hypointense or isointense signal on T2-weighted MRI sequences, reflecting hypercellularity and fibrosis. Laboratory evaluation frequently includes autoimmune panels, Erythrocyte Sedimentation Rate (ESR), and C-Reactive Protein (CRP) to assess systemic inflammatory or autoimmune disease. When tissue biopsy is obtained, histopathology typically demonstrates lymphoplasmacytic infiltrates with abundant IgG4-positive plasma cells, storiform fibrosis, obliterative phlebitis, and eosinophilic infiltration, consistent with an IgG4-related fibroinflammatory process [6,7].
Management is multidisciplinary and commonly involves ophthalmology, neurosurgery, otolaryngology, rheumatology, and radiation oncology. First-line treatment consists of corticosteroids, followed by steroid-sparing immunosuppressive agents such as methotrexate, azathioprine, mycophenolate mofetil, or rituximab. In cases refractory to medical therapy, surgical intervention and radiation therapy may be considered [8-10].
Radiation therapy has been infrequently reported in the treatment of IgG4-related pseudotumor and is generally regarded as a second-line option following failure of medical management [11,12]. In this paper, we present a case series of two patients with skull base pseudotumor treated with radiation therapy, demonstrating effective disease control, symptom improvement, and minimal toxicity at a single academic institution (XXX) between 1984 and 2024.
A 56-year-old woman presented with a one-year history of left ear fullness that developed following a dental extraction. Her symptoms have progressed to include headaches, low-grade fevers, and neck stiffness. She underwent an emergent left mastoidectomy with debridement, which revealed fibrous inflammatory tissue within the mastoid region. Postoperatively, she received six weeks of intravenous antibiotic therapy for presumed mastoiditis.
Four months after the initial surgery, the patient developed recurrent left ear fullness, temporal discomfort, and proptosis of the left ear. Computed Tomography (CT) demonstrated erosion of the left posterior fossa dura with a mass-like process involving the left mastoid. She subsequently underwent a second emergent mastoidectomy. Surgical pathology again demonstrated fibrosis with lymphoplasmacytic inflammation. Immunohistochemical stains were negative for melanoma (S-100) and sarcoma. This was followed by an additional prolonged course of intravenous and oral antibiotics, for a total antibiotic duration of approximately 3-4 months. Further evaluation, including lymphoma panel, infectious workup (bacterial and fungal cultures), and autoimmune studies, was negative. Despite this, the patient continued to have persistently elevated C-Reactive Protein (CRP) levels.
Approximately one year after her initial presentation, the patient experienced recurrence of left ear fullness, intermittent otorrhea, neck stiffness, and low-grade fevers. By this time, she had completed left-sided hearing loss, without evidence of involvement of other cranial nerves. A trial of oral corticosteroids (dexamethasone) failed to provide symptom relief.
Magnetic Resonance Imaging (MRI) of the head with and without contrast demonstrated confluent enhancing abnormal tissue within the mastoidectomy defect and middle ear, with disruption of the temporal bone posterior to the mastoid resection and medial to the otic capsule, as well as involvement of the left middle cranial fossa dura.
The case was reviewed at a multidisciplinary institutional tumor board involving otolaryngology and radiation oncology. The patient was deemed not to be a candidate for further surgical intervention. Consensus recommendation was for radiation therapy to achieve symptom relief, halt disease progression, and provide local control of the lymphoplasmacytic infiltrative process.
The patient was treated with external beam radiation therapy using Intensity-Modulated Radiation Therapy (IMRT) delivered via Volumetric Modulated Arc Therapy (VMAT), with daily Image-Guided Radiation Therapy (IGRT) using Cone-Beam Computed Tomography (CBCT). The treatment volume encompassed the post-surgical bed and MRI enhancing abnormal tissue around with an appropriate margin. A total dose of 4000 cGy was delivered in 20 fractions. Dosimetric parameters included D99% of 96.5%, D95% of 4434 cGy, and V100% of 99.9%, while respecting all Organ-at-Risk (OAR) constraints. Maximum doses to critical structures were as follows: optic chiasm 4089 cGy, left optic nerve 2252 cGy, right optic nerve 1285 cGy, and brainstem 4203 cGy (Figure 1).
At a follow-up duration of 76 months following completion of radiation therapy, the patient remained clinically stable without recurrence of left ear fullness, neck stiffness, otorrhea, or development of new neurological symptoms. She experienced no clinically significant radiation-related toxicities, including dermatitis, mucositis, or radiation necrosis. Surveillance MRI of the head performed annually for seven years demonstrated complete resolution of the previously noted granulation tissue, with no evidence of disease progression or recurrence (Figure 2).
A 69-year-old man with multiple medical comorbidities, including diabetes mellitus and a hypercoagulable state, presented with a six-month history of progressive hearing loss. Audiologic evaluation demonstrated mixed hearing loss. He referred to otolaryngology, where clinical examination revealed a soft tissue lesion involving the right external auditory canal. Biopsy of the lesion was negative for malignancy. A trial of oral corticosteroids was initiated but did not result in symptom improvement.
The patient subsequently underwent a right mastoidectomy. Surgical pathology demonstrated fragments of skin and viable bone with marked acute inflammation, granulation tissue, and fibrosis, findings consistent with IgG4-related pseudotumor. One month postoperatively, the patient developed right-sided facial palsy and intractable otalgia. Medical management with gabapentin was attempted; however, his neuropathic pain remained poorly controlled.
Over time, the patient experienced progression to multiple cranial neuropathies, including right vocal cord paralysis, worsening right facial weakness, and further decline in right-sided hearing. Comprehensive evaluation, including autoimmune panel, lymphoma panel, and infectious workup, was negative. He was evaluated by rheumatology and initiated on rituximab therapy without meaningful clinical improvement.
Magnetic Resonance Imaging (MRI) of the head with and without contrast demonstrated ill-defined soft tissue thickening and enhancement involving the bilateral nasopharyngeal and parapharyngeal spaces, as well as the right retro auricular and occipital scalp regions. Additionally, there was abnormal marrow signal and enhancement of the bilateral occipitotemporal skull base, more pronounced on the right.
The case was reviewed at the institutional multidisciplinary tumor board, including otolaryngology and radiation oncology. The clinical picture was consistent with IgG4-related pseudotumor involving the right temporal bone with associated progressive polycranial neuropathies, refractory to surgical resection and immunosuppressive therapy. Multidisciplinary consensus recommended radiation therapy for symptom palliation, halting disease progression, and achieving local control of the lymphoplasmacytic infiltrative process.
The patient subsequently underwent radiation therapy at his local institution using Intensity-Modulated Radiation Therapy (IMRT) with daily Image-Guided Radiation Therapy (IGRT) utilizing Cone-Beam Computed Tomography (CBCT). The treatment volume included the post-surgical bed with an appropriate margin. A total dose of 3000 cGy was delivered in 15 fractions. Dosimetric parameters included D99% of 92.2%, D95% of 96%, and V95% of 95.31%, while meeting all organ-at-risk (OAR) constraints. Maximum doses to critical structures were as follows: optic chiasm 502.5 cGy, left optic nerve 885.9 cGy, right optic nerve 838.7 cGy, and brainstem 3046 cGy.
Following radiation therapy, the patient experienced improvement in symptoms, and follow-up MRI performed six months post-treatment demonstrated stable granulomatous disease without evidence of progression. He did not develop radiation-related toxicities, including dermatitis or radiation necrosis. Unfortunately, the patient later developed cerebral venous thrombosis related to his underlying comorbid conditions and subsequently died.
Pseudotumor of the skull base, also referred to as immunoglobulin G4–related skull base disease represents a diagnostically and therapeutically challenging fibroinflammatory condition. First-line management typically consists of systemic corticosteroids, often followed by immunosuppressive or biologic agents such as rituximab. While many patients initially respond to medical therapy, a subset develops steroid-refractory, recurrent, or progressive disease requiring alternative treatment strategies.
In patients with rapidly progressive disease, multiple recurrences, or debilitating symptoms, radiation therapy should be considered as an effective option to achieve prompt symptom relief with acceptable toxicity. In select clinical scenarios, radiation therapy may provide a more expedient and durable response compared with prolonged immunosuppressive therapy, particularly when medical management fails or is poorly tolerated [13].
Certain histological subtypes, particularly those with prominent sclerosing features, have been shown to be less responsive to corticosteroids alone. In such cases, a combined approach incorporating surgical debulking followed by radiation therapy may be required to achieve adequate symptom control and prevent disease progression [14].
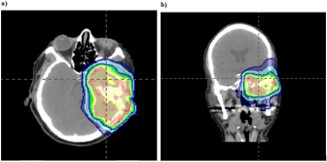
Figure 1: Radiation treatment plan for case 1. Intensity-Modulated Radiation Therapy (IMRT) delivered using Volumetric Modulated Arc Therapy (VMAT) demonstrating target volume coverage of the post-surgical skull base region while respecting adjacent organs at risk. (A) Axial view (B) Coronal view.
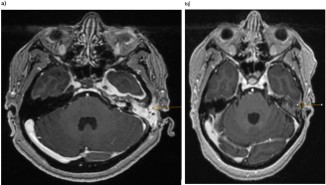
Figure 2: Magnetic resonance imaging of Case 1 before and after radiation therapy. Axial T1-weighted post-contrast MRI images demonstrating: (A) Pre-radiation therapy imaging obtained on 08/16/2018, showing enhancing fibroinflammatory tissue within the left mastoidectomy bed and adjacent skull base structures. (B) post-radiation therapy imaging obtained on 12/02/2024, demonstrating resolution of previously noted enhancement with no evidence of disease progression.
Prior literature has reported radiation doses ranging from 2000-3000 cGy, typically delivered in 200 cGy per fraction, with overall response rates of approximately 75-93% and complete response rates of 35-45%. Radiation therapy has been associated with rapid improvement in symptoms in 81-87% of patients, frequently allowing reduction or discontinuation of chronic corticosteroid therapy in steroid-dependent individuals [12,15].
Radiation therapy is generally well tolerated, with reported acute toxicities including fatigue, localized alopecia, and radiation dermatitis. Common late effects include radiation induced dry eye (approximately 10%) and cataract formation (10-35%). Rare but serious complications include radiation necrosis of the brain or brainstem, which may present tinnitus, headaches, or seizures and can be managed with corticosteroids and, in select cases, bevacizumab. Other uncommon risks include optic neuropathy resulting in visual deficits and cochlear injury leading to hearing loss. The use of modern radiation techniques such as Intensity-Modulated Radiation Therapy (IMRT) or Volumetric Modulated Arc Therapy (VMAT), combined with daily Image-Guided Radiation Therapy (IGRT) using cone-beam CT and strict adherence to Organ-at-Risk (OAR) dose constraints, has significantly reduced the incidence of these toxicities. Additionally, select reports have described re-irradiation in patients with orbital pseudotumor, with acceptable toxicity when cumulative OAR doses are calculated and respected [12,15].
Most previously published series describe treatment with doses of 2000-3000 cGy. In contrast, our institutional experience includes two patients treated with 4000 cGy in 20 fractions and 3000 cGy in 15 fractions, respectively, without evidence of optic apparatus toxicity, radiation necrosis, or other significant late effects [11,12,15]. Both patients had pathologically confirmed IgG4-related disease, underwent multidisciplinary evaluation involving otolaryngology, pathology, radiology, ophthalmology, rheumatology, and radiation oncology, and had disease refractory to medical management and surgical intervention. Following radiation therapy, both patients experienced meaningful and durable improvement of the symptoms with excellent local control.
Although limited by the small number of patients, this case series supports the role of radiation therapy as a safe and effective treatment option for refractory IgG4-related pseudotumor of the skull base and orbit. Radiation therapy should be considered earlier in the disease course for patients with progressive symptoms, cranial neuropathies, or steroid-refractory disease, particularly within the context of multidisciplinary decision making.
In patients with IgG4-related pseudotumor of skull base with diffuse involvement of the optic nerve, mastoid, or dura and severe symptoms such as vision or hearing loss, chronic otorrhea, and intractable pain, disease control may not be achievable with medical therapy or surgical intervention alone. A short course of radiation therapy delivered with modern techniques such as Intensity-Modulated Radiation Therapy (IMRT) and daily Image-Guided Radiation Therapy (IGRT) using cone-beam CT can provide effective local control, durable symptom relief, and progression-free survival with minimal treatment-related toxicity. Radiation therapy should be considered a valuable therapeutic option in the multidisciplinary management of refractory IgG4-related disease.
Human subjects: This study (STUDY00141133) received a waiver under IRB00000161 U of Kansas Med Ctr IRB #1 – Kansas City campus Institutional Review Board (IRB).
Declaration of generative AI and AI-assisted technologies in the writing process: During the preparation of this work the author(s) used Large Language Models (LLMs) for language editing and clarity. After using this tool, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Data sharing statement: All data generated have been included in this manuscript.