Article Type: Research Article, Volume 3 Issue 1
*Corresponding author: Mawuli AK Santos
Department of Ophthalmology, Faculty of Health Sciences, Université de Lomé, Togo.
Email: santosmawuli@yahoo.fr
Received: Feb 03, 2026 Accepted: Feb 18, 2026 Published: Feb 25, 2026
Citation: Santos MAK, Nagbe YE, Dzidzinyo K, Manhe N, Vonor K, et al. Intracular pressure and central corneal thickness profile in non-glaucomatous subjects with melanoderma in Togo. Ann Case Rep Med Images. 2026; 3(1): 1069.
Copyright: Santos MAK et al. © All rights are reserved
Purpose: To describe Intraocular Pressure (IOP) and Central Corneal Thickness (CCT) profiles in non-glaucomatous melanodermic subjects in Togo.
Methods: This retrospective descriptive study included all non-glaucomatous melanodermic patients examined at the Ophthalmology Department of the Centre Hospitalier des Armées, Lomé, between July 2017 and June 2022. Patients underwent a complete ophthalmologic examination, including IOP and CCT measurements using a NIDEK tonopachymeter. Exclusion criteria were glaucoma, ocular trauma, uveitis, corticosteroid therapy, or significant corneal pathology. Collected data included age, sex, uncorrected and pachymetry-corrected IOP, and CCT of both eyes.
Results: A total of 350 patients (700 eyes) were included: 201 men and 149 women, mean age 36.7±14.5 years. Mean uncorrected IOP was 14.38±3.24 mmHg in the right eye and 14.19±3.18 mmHg in the left eye. Mean CCT was 539.8±35.3 µm in the right eye and 536.3±33.3 µm in the left eye, decreasing progressively after 20 years (p=0.0087). Pachymetry-corrected IOP was 14.86±3.00 mmHg in the right eye and 14.82±2.98 mmHg in the left eye, increasing with age, particularly after the second decade.
Conclusion: In non-glaucomatous melanodermic subjects, CCT decreases and IOP increases with age. Systematicpachymetry allows more accurate assessment of IOP and may improve glaucoma risk evaluation.
Keywords: Intraocular pressure; Central corneal thickness; Pachymetry; Melanoderma.
Intraocular Pressure (IOP) is a major diagnostic and prognos- tic factor in glaucoma management [1]. However, measured IOP values are influenced by Central Corneal Thickness (CCT), which can lead to underestimation or overestimation of true IOP. Pachymetry is therefore essential for accurate interpretation of IOP and for calculating pachymetry-corrected IOP.
Several studies conducted outside Africa have shown that individuals with melanoderma tend to have higher IOP values [2] and thinner corneas compared with Caucasian populations [3-5]. These anatomical and physiological differences may contribute to a poorer prognosis of glaucoma in dark-skinned populations. In sub-Saharan Africa, however, data on CCT and corrected IOP in melanodermic subjects remain limited. Available studies have reported thinner corneas compared with global reference values [6,7], but regional data are still scarce.
In Togo, previous studies have focused on glaucomatous and non-glaucomatous populations by assessing either uncorrected IOP [8,9] or CCT alone [10]. To date, few studies have simulta- neously evaluated uncorrected IOP, pachymetry-corrected IOP, and CCT in non-glaucomatous melanodermic subjects.
The aim of this study was therefore to determine the profiles of uncorrected and corrected IOP as well as CCT in non-glauco- matous melanodermic subjects examined in Lomé, Togo.
Study design and population
This retrospective descriptive study was conducted in the ophthalmology department of the Centre Hospitalier des Ar- mées de Lomé, Togo, over a five-year period from July 2017 to June 2022.
We included melanodermic patients of all ages who under- went a complete ophthalmological examination, including In- traocular Pressure (IOP) measurement and pachymetry. Only non-glaucomatous subjects were included, defined by a fundus examination showing a vertical cup-to-disc ratio ≤0.3.
Patients were excluded if they had a diagnosis of glaucoma, were receiving topical or systemic corticosteroid therapy, had a history of recent ocular trauma or uveitis, or presented with a cup-to-disc ratio >0.3. Patients with stage III pterygium, central corneal scarring, or corneal edema were also excluded.
Data collection and variables
Data were collected retrospectively from medical records us- ing a standardized data collection form. The variables analyzed included age, sex, uncorrected IOP and pachymetry-corrected IOP in both eyes, and Central Corneal Thickness (CCT) in both eyes.
IOP and CCT measurements were performed using a NIDEK tonopachymeter. This non-contact device measures IOP by air- puff tonometry and CCT by integrated pachymetry. Pachymetry- corrected IOP values were automatically provided by the device based on an internal compensation algorithm. IOP values were expressed in millimeters of mercury (mmHg) and CCT values in micrometers (µm).
Statistical analysis and ethical considerations
Data entry was performed using EpiData version 3.1, and sta- tistical analysis was carried out with RStudio software. Quanti- tative variables were compared using Student’s t-test or Analy- sis of Variance (ANOVA), as appropriate. Correlations between quantitative variables were assessed using correlation tests. A p-value<0.05 was considered statistically significant.
This study was approved by the hospital administration, and all collected data were handled confidentially in accordance with ethical standards.
A total of 350 melanodermic patients, corresponding to 700 eyes, were included in the study. There were 201 men and 149 women, yielding a male-to-female ratio of 1.35. The mean age was 36.72±14.48 years (range: 7-81 years). The 40-50 year age group was the most represented (Figure 1).
Uncorrected intraocular pressure
Mean uncorrected IOP in the right eye was 14.38±3.24 mmHg (range: 7.7-25.7 mmHg), compared with 14.19±3.18 mmHg (range: 7.3-25 mmHg) in the left eye. The difference be- tween eyes was statistically significant (p<0.0001). The overall mean uncorrected IOP was 14.28±3.07 mmHg. Mean IOP was 14.26 mmHg in men and 14.32 mmHg in women, with no statis- tically significant difference (p=0.8689).
Uncorrected IOP was highest in children under 10 years of age (15.58 mmHg), decreased until the 20-30-year age group, and subsequently increased progressively with age, reaching its highest values in patients aged 60 years and older (p=0.047) (Figure 2). The most frequent IOP range was 10-15 mmHg, ob- served in 64.86% of right eyes and 68.29% of left eyes (Table 1).
Central corneal thickness
Mean CCT was 539.78±35.33 µm (range: 450-632 µm) in the right eye and 536.30±33.29 µm (range: 453-634 µm) in the left eye. The difference between eyes was statistically significant (p<0.0001). The overall mean CCT was 538.54±33.28 µm.
Mean CCT was 539.48 µm in men and 536.11 µm in women, with no statistically significant difference (p=0.3501). CCT was highest in the 10-20-year age group (548.66 µm) and showed a progressive decrease with age, reaching its lowest values in patients aged 60 years and older (p=0.0087) (Figure 3).
Pachymetry-corrected intraocular pressure
Mean pachymetry-corrected IOP was 14.86±3.00 mmHg (range: 8.86-25.8 mmHg) in the right eye and 14.82±2.98 mmHg (range: 7.9-25.3 mmHg) in the left eye. The difference between eyes was statistically significant (p<0.0001). The overall mean corrected IOP was 14.84±2.82 mmHg.
Mean corrected IOP was 14.72 mmHg in men and 15.02 mmHg in women, with no statistically significant difference (p=0.355). Corrected IOP increased progressively with age, with an average increase observed every 10 years starting from the 10-20-year age group (Figure 4).
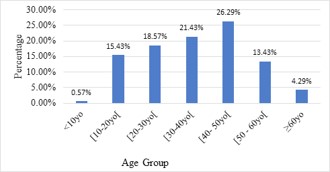
Figure 1: Patient distribution per age group.
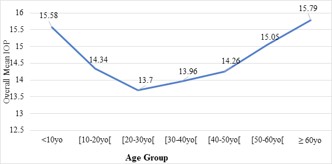
Figure 2: Variation in mean IOP by age group.
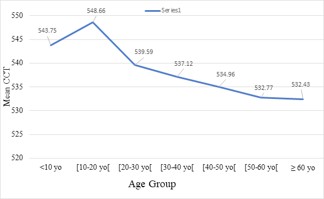
Figure 3: Variation in the overall mean CCT of both eyes per age group.
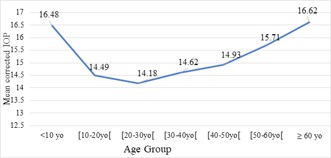
Figure 4: Variation in mean corrected IOP in both eyes per age group.
| Right eye | Left eye | |||
|---|---|---|---|---|
| n | % | n | % | |
| 5-9 mmHg | 24 | 6.86 | 21 | 6 |
| 10-15 mmHg | 227 | 64.86 | 239 | 68.29 |
| 16-21 mmHg | 89 | 25.43 | 84 | 24 |
| 22-28 mmHg | 10 | 2.85 | 6 | 1.71 |
| Total | 350 | 100 | 350 | 100 |
The mean age of patients in this study was 36.72±14.48 years, with a predominance of young adults. The 40-50-year age group was the most represented. Similar age distributions have been reported in studies conducted in sub-Saharan Afri- ca, notably in Cameroon and Côte d’Ivoire, where mean ages ranged from 31 to 44 years [6,11]. This reflects the demographic structure of these populations and the high ophthalmological consultation rate among young and middle-aged adults.
A male predominance was observed, with a male-to-female ratio of 1.35. Comparable findings have been reported in Côte d’Ivoire [12], whereas a female predominance was described in Cameroon [6]. These differences are likely related to variations in healthcare access and consultation patterns rather than true biological differences.
The mean uncorrected intraocular pressure in our study was 14.28±3.07 mmHg, with no significant difference between sex- es. These results are consistent with those reported by Eballe et al. [6], who found a mean uncorrected IOP of 13.01±2.97 mmHg in a non-glaucomatous Cameroonian population. As previously described, uncorrected IOP showed a significant association with age, with a progressive increase observed in older age groups.
After pachymetry correction, mean IOP increased to 14.84±2.82 mmHg across the study population. This systematic increase compared with uncorrected values highlights the influ- ence of corneal thickness on IOP measurement. Similar findings have been reported in melanodermic populations, with an av- erage increase in corrected IOP of approximately 2 to 3 mmHg [6,7,11-15]. In our study, corrected IOP increased progressively with age, particularly after 20 years, which is in agreement with previously published data.
The mean central corneal thickness was 538.54±33.28 µm, with no significant difference between sexes. This value is com- parable to those reported in other melanodermic populations in West and Central Africa [6,10,12]. In contrast, studies con- ducted in Caucasian and Asian populations have consistently reported thicker corneas, with mean CCT values generally ex- ceeding 555 µm [13,17,18]. These interethnic differences in cor- neal thickness may partially explain the higher risk and poorer prognosis of glaucoma observed in melanodermic subjects.
A statistically significant decrease in CCT with age was ob- served in our study, beginning after the age of 20. This finding is consistent with previous reports showing a progressive reduc- tion in CCT of approximately 2 to 3 µm per decade [3-5,19,20]. Age-related corneal thinning may contribute to underestima- tion of IOP in older patients if pachymetry is not routinely per- formed.
Overall, the combination of thinner corneas and higher cor- rected IOP values in melanodermic subjects underscores the importance of systematic CCT measurement in this population. Accurate assessment of IOP is essential for early detection, risk stratification, and optimal management of glaucoma, particu- larly in populations at increased risk.
In non-glaucomatous melanodermic subjects in Togo, cen- tral corneal thickness is relatively low and intraocular pressure is moderately elevated. Corneal thickness decreases and intra- ocular pressure increases with age, particularly after the third decade. These findings highlight the importance of systematic pachymetry for accurate assessment of intraocular pressure and glaucoma risk.
Conflict of interest: The authors declare no conflict of interest.
Funding: This study received no external funding.