Article Type: Research Article, Volume 3 Issue 1
*Corresponding author: Mawuli AK Santos
Department of Ophthalmology, Faculty of Health Sciences, Université de Lomé, Togo. BP: 30256 Lomé, Togo.
Email: santosmawuli@yahoo.fr
Received: Feb 03, 2026 Accepted: Feb 18, 2026 Published: Feb 25, 2026
Citation: Santos MAK, Dzidzinyo K, Prempe YS, Maneh N, Vonor K, et al. Epidemiological profile of distance visual impairment among adults aged 50 years and older in Northern Togo in 2024. Ann Case Rep Med Images. 2026; 3(1): 1068.
Copyright: Santos MAK et al. © All rights are reserved
Objective: To describe the epidemiological profile of distance visual impairment among individuals aged 50 years and older in northern Togo in 2024.
Methods: A cross-sectional, RAAB (Rapid Assessment of Avoidable Blindness) survey was conducted from November to December 2024 among residents aged ≥50 years. Sociodemographic, clinical, and functional data were collected. Distance visual acuity was measured uncorrected, with a pinhole, and with corrective lenses if needed. Causes of visual impairment were determined following the RAAB methodology.
Results: A total of 4,290 participants were included (mean age 63.1±10.4 years; male-to-female ratio 0.57). Visual impairment was present in 40.8% of participants. The leading causes were cataract (49.7%) and uncorrected refractive errors (34.6%). Visual impairment was significantly associated with age, sex, and socioeconomic status (p<0.001). Cataract surgical coverage was 26.5%, with an effective coverage of 17%. Major barriers to surgery included low socioeconomic status and lack of awareness of treatment. Most visually impaired participants reported anxiety related to poor vision.
Conclusion: Distance visual impairment remains common among the elderly in northern Togo but is largely preventable. Strengthening screening, access to corrective lenses, and cataract surgery is essential.
Keywords: Visual impairment; Elderly; Cataract; Refractive error; Togo.
Visual impairment is a major public health problem, particularly among older adults. Recent data remain scarce in some regions of Togo, especially in rural and hard-to-reach areas of the northern part of the country.
According to the World Health Organization (WHO) World Report on Vision, visual impairment is defined as a best-eye distance visual acuity of less than 5/10 [1]. Globally, at least 2.2 billion people live with some form of visual impairment, a large proportion of which is preventable or correctable [1].
In sub-Saharan Africa, the prevalence of visual impairment ranges from 10% to 17%, while blindness affects between 1.2% and 3.4% of the population [2,3]. In Togo, the 2014 Rapid Assessment of Avoidable Blindness (RAAB) survey estimated the prevalence of visual impairment at 20.8% among adults aged 50 years and older [4]. However, updated epidemiological data, particularly in northern rural regions, remain limited.
An up-to-date understanding of the epidemiological profile of distance visual impairment among older adults is essential for guiding prevention, screening and management strategies. This study aimed to describe the epidemiological profile of distance visual impairment among adults aged 50 years and older in northern Togo in 2024.
Study design and setting
A cross-sectional descriptive study using the Rapid Assessment of Avoidable Blindness (RAAB) methodology was conducted from November to December 2024 in northern Togo. A two-stage cluster sampling method was used, in accordance with RAAB guidelines, to ensure representativeness of the population aged 50 years and older.
Study population
All men and women aged 50 years and older who had been residing for at least six months in a household in northern Togo and who provided informed consent were included. Individuals living in institutions, those younger than 50 years, or those unable to respond to the survey were excluded.
Data collection
Field surveys were conducted by trained teams consisting of an ophthalmologist, an ophthalmic technician, a local guide and a driver. Distance visual acuity was measured without correction using standard RAAB charts. For visual acuity <5/10, pinhole testing was performed, and participants wearing distance correction were retested with their habitual correction. Anterior segment examination was performed using a slit lamp, and fundus examination was carried out after pupillary dilation.
Operational definitions
Visual impairment was defined as best-eye visual acuity
<5/10 and classified according to the ICD-11. Uncorrected visual acuity was prioritized in order to better reflect unmet needs for eye care services within the community. According to RAAB methodology, only one principal cause of visual impairment, the most easily treatable, was assigned per participant.
Statistical analysis
Data were entered using RAAB software version 7 and analyzed with Microsoft Excel 2019 and R software version 4.0.4. Associations were assessed using appropriate statistical tests, with p<0.05 considered statistically significant.
Ethical considerations: Confidentiality and anonymity of participants were respected in accordance with ethical principles.
Sociodemographic characteristics
A total of 4,290 participants were included, with a participation rate of 99.8%. The mean age was 63.1±10.4 years (range: 50-102 years). Women accounted for 63.8% of the sample (male-to-female ratio=0.57). The age group 50-59 years was the most represented (42.0%). The distribution of participants by age group and sex is presented in (Table 1).
Nearly half of households (48.3%) had a monthly income below the national minimum wage, indicating a predominantly low socioeconomic status. The distribution of households according to income level is shown in (Table 2).
Prevalence and causes of visual impairment
Distance visual impairment was identified in 1,752 participants, corresponding to a prevalence of 40.8% (Figure 1). Cataract was the leading cause (49.7%), followed by uncorrected refractive errors (34.6%) (Figure 2). Other causes accounted for a smaller proportion of cases. Visual impairment was significantly associated with age, sex and socioeconomic status (p<0.001).
Cataract surgery
Cataract surgery had been performed in 313 participants (7.3%), with a mean age at surgery of 68.6±10.5 years. The characteristics of cataract surgery, including age at surgery, place of intervention, surgical technique and cost, are summarized in (Table 3).
Overall cataract surgical coverage was estimated at 26.5%. Among operated individuals, 68.4% still presented with visual impairment, resulting in an effective cataract surgical coverage of 17%. Uncorrected refractive errors were the leading cause of postoperative poor visual outcome (32.6%) (Figure 3).
Psychological impact
Among participants with visual impairment (n=1,752), only 9.7% reported maintaining good morale despite poor vision. The remaining participants reported varying frequencies of anxiety related to their visual condition, ranging from occasional to daily anxiety. The distribution of anxiety frequency among visually impaired participants is presented in (Table 4).
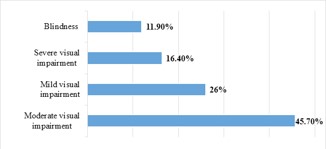
Figure 1: Prevalence of distance visual impairment among adults aged 50 years and older.
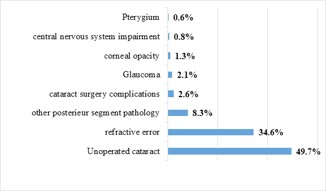
Figure 2: Distribution of the main causes of distance visual impairment.
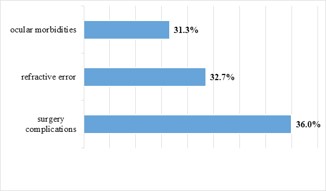
Figure 3: Causes of poor visual outcome after cataract surgery.
| Female | Male | Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 50-59 years | 1120 | 40,9 | 681 | 43,9 | 1801 | 42,0 |
| 60-69 years | 833 | 30,4 | 497 | 32,0 | 1330 | 31,0 |
| 70-79 years | 503 | 18,4 | 249 | 16,0 | 752 | 17.5 |
| ≥ 80 years | 282 | 10,3 | 125 | 8,1 | 407 | 9.5 |
| Total | 2738 | 100,0 | 1552 | 100 | 4290 | 100,0 |
| n | % | |
|---|---|---|
| Insufficient | 2073 | 48,3 |
| Fair | 1755 | 40,9 |
| Adequate | 273 | 6,4 |
| Good | 182 | 4,2 |
| Excellent | 7 | 0,2 |
| Total | 4290 | 100 |
| n | % | |
|---|---|---|
| Age at the Time of Surgery (years) (313) | ||
| < 40 | 1 | 0,3 |
| 40-49 | 2 | 0,6 |
| 50-59 | 54 | 17,3 |
| 60-69 | 104 | 33,2 |
| 70-79 | 106 | 33,9 |
| 80-89 | 36 | 11,5 |
| 90-99 | 10 | 3,2 |
| Place of surgery (313) | ||
| Public hospital | 210 | 67,0 |
| Ophthalmologic camp / Makeshift setting | 59 | 18,9 |
| Volunteer / Charitable hospital | 31 | 9,9 |
| Private hospital | 8 | 2,6 |
| Traditional setting | 5 | 1,6 |
| Type of surgery (313) | ||
| Surgery with intraocular lens (IOL) | 299 | 95,5 |
| Couching | 4 | 1,3 |
| No IOL inserted | 10 | 3,2 |
| Cost of surgery (313) | ||
| Completely free | 225 | 71,9 |
| Fully paid | 68 | 21,7 |
| Partially free | 20 | 6,4 |
| n | % | |
|---|---|---|
| Never | 170 | 9,7 |
| A few times per year | 874 | 49,9 |
| Monthly | 483 | 27,6 |
| Weekly | 200 | 11,4 |
| Daily | 25 | 1,4 |
This study highlights a high prevalence of distance visual impairment (40.8%) among adults aged 50 years and older in northern Togo. This prevalence is higher than that reported in several RAAB surveys conducted in sub-Saharan Africa, including Mali (27.7%) and Nigeria (27.5%) [5,6]. These differences may be explained by variations in visual impairment definitions, the use of uncorrected visual acuity in the present study, and disparities in access to eye care services.
Cataract and uncorrected refractive errors remain the leading causes of visual impairment, confirming their predominance among avoidable causes in low and middle-income countries. These findings are consistent with reports from West Africa and global WHO estimates indicating that cataract and refractive errors account for more than 70% of avoidable visual impairment [1,6,7].
The significant association between visual impairment and age reflects physiological ocular aging and the accumulation of chronic diseases with advancing age [8]. Female predominance is in line with demographic data showing higher life expectancy among women, increasing their exposure to age-related conditions [9]. The association with low socioeconomic status underscores the role of social inequalities in access to eye care services [10].
Cataract surgical coverage remains insufficient, although comparable to that reported in neighboring countries [9,11]. The high proportion of postoperative visual impairment highlights the importance of surgical quality, postoperative follow-up and systematic refractive correction after surgery.
Study limitations
This study has some limitations. The RAAB methodology allows attribution of only one main cause of visual impairment per participant, which may underestimate coexisting ocular pathologies. Visual acuity assessment was limited to distance vision and did not include evaluation of postoperative visual quality or patient-reported outcomes. In addition, the cross-sectional design does not allow causal inference.
From a public health perspective, the main barriers identified poverty and lack of awareness of available treatment have also been reported in Togo and neighboring countries [9,12]. The psychological burden associated with visual impairment, marked by anxiety, confirms that vision loss is not only a functional limitation but also a major psychosocial issue [13,14].
In the context of demographic transition and progressive population aging in Togo, these results support the strengthening of national eye health policies in line with the global initiative “Vision 2030”.
Distance visual impairment among adults aged 50 years and older in northern Togo is common and largely avoidable. Strengthening screening programs, improving access to refractive services and cataract surgery, ensuring systematic postoperative refractive correction, and enhancing community awareness are essential actions to reduce the burden of visual impairment. These measures should be integrated into national eye health strategies in line with the objectives of the global Vision 2030 initiative.
Authors’ contributions: All authors contributed to the conception and design of the study, data collection, analysis and interpretation of the results. All authors participated in drafting and revising the manuscript and approved the final version.
Funding: The survey was conducted under the supervision of the National Eye Health Program and funded by the German Cooperation (BMZ) and Christian Blind Mission (CBM).
Conflicts of interest: The authors declare no conflicts of interest.