Article Type: Short Report, Volume 3 Issue 1
*Corresponding author: Emin BODAKÇİ
Gaziantep City Hospital Gastroenterology Clinic, Turkiye.
Email: doktor.emin.0903@hotmail.com
Received: Jan 10, 2026 Accepted: Feb 06, 2026 Published: Feb 13, 2026
Citation: Bodakci E. Herpes simplex virus-1 associated esophagitis concomitant with gastritis in an immunocompetent host. Ann Case Rep Med Images. 2026; 3(1): 1065.
Copyright: Bodakci E © All rights are reserved
Herpes Simplex Virus (HSV) esophagitis is the most common viral esophagitis in clinical practice [1]. Herpes Esophagitis (HE) is typically caused by Herpes Simplex Virus type 1 (HSV-1), although less frequently, it is caused by HSV type 2 (HSV-2). Most cases of HE occur in immunocompromised hosts, but occasionally immunocompetent patients develop this condition [2]. Common risk factors for HE include a history of HIV, AIDS, malignancy, solid organs transplant, use of steroids, immuno-suppressant medications, chemotherapy, and radiation therapy [2-4]. This article presents a case of a 50-year-old woman who was using steroids for rheumatoid arthritis and developed HSV esophagitis concominant gastritis.
A 50-year-old female patient presented to our outpatient clinic with odynophagia, dysphagia, and excessive salivation ex-tending from the throat to the epigastric region, lasting for two weeks. Her medical history revealed a history of rheumatoid arthritis, followed for approximately three years, during which she received leflunomid treatment. She stated that she had started oral methylprednisolone treatment one month prior due to disease activation, and that her symptoms began after this treatment. Her vital signs and physical examination were normal. The patient’s laboratory values showed no significant findings except for White Blood Cell (WBC) 13,500 (4-10,000) and C-Reactive Protein (CRP) elevation above 10 mg/L (0-5). Upper gastrointestinal endoscopy revealed deep, fissured ulcerations with volcano-like craters, 3-7 mm in diameter, start-ing from the proximal esophagus and continuing throughout the esophagus (Figure 1). The ulcers were observed to continue throughout the stomach, but were more superficial (Figure 2). Biopsies were taken from the patient with a diagnosis of viral esophagitis and gastritis. Viral serology was performed on the patient. Serology for Human Immunodeficiency (HIV), Cyto-megalovirus (CMV), Epstein-Barr virus, and Herpes Simplex Virus (HSV 1-2) was tested. HSV-1 IGM serology was reported as positive. Biopsies revealed a dense mix of inflammatory cells infiltrating the epithelium, and epithelial cells containing intra-nuclear inclusions among multinuclear giant cells (Figure 3). The intranuclear inclusions were surrounded by a halo. The viral cytopathic effect was consistent with herpes simplex virus. The patient was started on intravenous acyclovir 3×5 mg/kg with a preliminary diagnosis of HSV esophagitis and gastritis. On the 3rd day, the patient’s symptoms subsided, and they were dis-charged with oral acyclovir. A follow-up endoscopy performed on the 22nd day after 2 weeks of treatment showed complete healing of the lesions in the esophagus and stomach without any sequelae.

Figure 1: Volcano like ulcer in the esophagus.
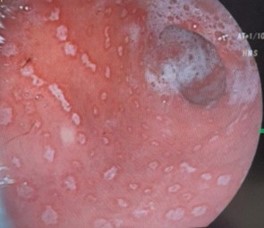
Figure 2: HSV induced in the stomach.
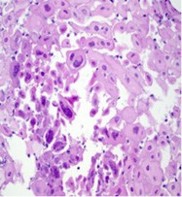
Figure 3: Intranuclear inclusions among multinuclear giant cells.
HSV esophagitis is a well-known disease in immunocompromised hosts, which can happen as a primary infection or as a reactivation of a latent virus [5]. On the other hand, HSV infections in the stomach and the duodenum are much less common than those in the esophagus, rectum, and perineum [6]. Most cases of HSV esophagitis are due to HSV-1, but a few case reports of HSV-2 esophagitis have been described. Patients usually have a prodromal systemic manifestation of fever, nausea, or vomiting before manifesting esophageal symptoms. The most common symptoms are odynophagia, dysphagia, heart-burn, epigastric pain, or chest pain. Concurrent oropharyngeal lesions are uncommon in immunocompetent hosts, but immunocompromised hosts usually have co-existent herpes labialis or oropharyngeal ulcers [7,8]. Our case is one of the few reported cases in the literature of concominant HSV esophagitis and gastritis. In an immunocompromised patient, the development of dysphagia should raise suspicion of infective esophagitis. The three most common causes of infective esophagitis are HSV, Candida albicans, and CMV. HSV esophagitis can cause dysphagia, odynophagia, or gastrointestinal bleeding. Endoscopy may reveal nonspecific inflammation, separate ulcers, superficial ulcers, or pseudomembranous esophagitis. Biopsy findings are very helpful in diagnosis.
The diagnosis of HSV esophagitis is usually based on endoscopic findings confirmed by histopathological examination. Endoscopic findings include friable mucosa with numerous well-circumscribed ulcers smaller than 2 cm, most commonly in the distal esophagus [1]. The margin of an ulcer, where viral cytopathic activity is most likely to be noticed, should be the lo-cation of biopsies. Multinucleated giant cells with ground-glass nuclei and eosinophilic inclusions are examples of histologic findings. Additionally helpful may be an immunohistochemical analysis for HSV glycoproteins [9]. In our case, endoscopy revealed characteristic ulcers in the esophagus and stomach, and serology showed HSV type-1 IGM positivity. Intranuclear inclusion bodies and multinuclear giant cells were observed in the biopsy samples.
Our case is one of HSV-induced esophagitis and concomitant gastritis developing after anabolic steroid use, and complete recovery was achieved with discontinuation of steroid treatment and acyclovir therapy.