Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Luigi Rigacci
Research Unit of Hematology and Stem Cell Transplantation, Department of Medicine and Surgery, Università Campus BioMedico di Roma, Italy.
Email: l.rigacci@policlinicocampus.it
Received: Dec 23, 2025 Accepted: Jan 21, 2026 Published: Jan 28, 2026
Citation: Teresa A, Federico V, Elisabetta C, Antonella B, Francesco G, et al. Splenic rupture after ibrutinib discontinuation. Ann Case Rep Med Images. 2026; 3(1): 1063.
Copyright: Rigacci L et al. © All rights are reserved
Chronic Lymphocytic Leukemia (CLL) is the most prevalent leukemia in adults in Western Countries. Remarkable strides have been achieved in treatment of CLL. One notable class of agents revolutionizing CLL treatment is Bruton’s Tyrosine Kinase Inhibitors (BTKi), which have reshaped the landscape by proving viable alternatives to traditional chemotherapy and immunotherapy. The BTKi are indicated both in relapsed/refractory and at first line setting patients. The first-in-class BTKi, Ibrutinib, is generally administered until disease progression or until unacceptable toxicity. Despite Ibrutinib is considered easy manageable and well-tolerated drug, instances of discontinuation are not uncommon. The most frequent reason leading to ibrutinib discontinuation are infections. Drug discontinuation could determine a quick arise in lymphocyte count and their migration in lymphoid organs leading to a rapid progression of the disease, characterized by the recurrence of general symptoms and a rapid worsening of lymphadenopathy or splenomegaly. In real life settings it has been documented a rapid drop of lymphocyte count attributable to the migration of lymphocyte to the spleen. which could represent a potential cause for splenic infarction and rupture. We reported the case report of a patient who discontinued Ibrutinib due to pulmonary infection. Subsequently, the patient experienced a life-threatening episode of splenic rupture, underscoring the critical considerations surrounding the discontinuation of such targeted therapies in the management of CLL.
Chronic Lymphocytic Leukemia (CLL) is the most prevalent leukemia in adults in Western Countries [1]. Over the past de-cades significant development was made in treatment strate-gies in CLL. Novel target agents, including Bruton’s Tyrosine Ki-nase Inhibitors (BTKi), have changed the CLL treatment scenario without using chemotherapy and immunotherapy, indicated both in relapsed/refractory and at first line setting patients [2,3]. The first-in- class BTKi, Ibrutinib, irreversibly inhibits B-cell’s BTK intracellular pathway, impeding CLL cells migration and adhesion from peripheral blood to lymphoid tissues (lead-ing to an expected transient early-phase therapy lymphocyto-sis), proliferation and interaction with tumor microenvironment [4]. Treatment with Ibrutinib should be continued until disease progression or unacceptable toxicity [5]. Despite Ibrutinib is considered easy to handle and well tolerated drug, discontinu-ing therapy is not so rare.
The most frequent reason leading to ibrutinib discontinua-tion can be disease progression, Richter syndrome, atrial fibril-lation, bleeding, infections and second malignancies.
The rate of discontinuation because of adverse events is most frequent during the first year of ibrutinib treatment and generally decreased over time [2].
Serious Infections are among the most frequent treatment-related adverse events. Between infections, pneumonia is more common in relapsed/refractory cases than in treatment-naïve patients who had been started on ibrutinib. However, several studies demonstrated that they can occur early on treatment after a median time of 7 months from starting ibrutinib. This observation suggests careful monitoring of patients during the first months [6-8].
Ibrutinib discontinuation could determine a lack of control in chemokine release and lymphocytes proliferation, determin-ing a quick rise in lymphocyte count and their migration in lym-phoid organs [9]. This could lead to a rapid disease progression or Richter’s transformation, in terms of reappearing of general symptoms, rapidly worsening of splenomegaly or lymphade-nopathy and progressively laboratory changes (rising lympho-cyte count or lactate dehydrogenase values) [10].
In real life settings it has been observed a rapid drop of lym-phocyte count depending on lymphocyte spleen migration, which could represent a risk factor for splenic infarction and rupture [9-11].
The case report we present refers to a 74-year-old man af-fected by CLL who presented acute splenic rupture after a tem-porarily cessation of ibrutinib.
The patient had the history of prostatic cancer treated with surgery and radiotherapy in 2013, relapsed in 2020 and treated with hormonal therapy. During oncologic follow-up no spleno-megaly or lymphocytosis were reported.
His hematological history started on June 10th, 2022, when he was admitted to the Emergency Room (ER), complaining of spread musculoskeletal pain. His blood investigations results were as follow: Hemoglobin (Hb) 9.5 gr/dl, White Blood Cor-puscles (WBC) 115.000/mmc with lymphocyte 105.000/mmc, platelet count 181.000/mmc, Lactate Dehydrogenase (LDH) 322 UI/L, hepatorenal chemistry within normal limits, direct and in-direct Coombs test were negative.
Computerized Tomography (CT) scan revealed splenomegaly with 25 cm of bipolar diameter (Figure 1), associated with sub and peri-centimetric lymphonodes above and below the dia-phragm and confluent celiac and periaortic lymphonodes (di-mensions 27×15 mm).

Figure 1: CT scan performed in July 2022 showing a spleen with a bipolar diameter of 25 cm.
Peripheral blood smear showed characteristically small, mature-appearing lymphocytes that raised 90% of the total cell count, several Gumprect’s nuclear shadows, few prolympho-cytes. Flow cytometry confirmed the diagnosis of CLL [94% of CD5/CD19 (+) cells displaying the following phenotype: CD19(+), CD5(+), CD20 (++), CD23 (+), CD79b(+), CD49d(+)(99%), with kappa monoclonality. Cytogenetic analysis revealed the dele-tions of 13q14. NGS technique revealed TP53 disruption and Immunoglobulin heavy chain variable region (IGHV) analysis demonstrates a not-mutated CLL clone.
In July, persisting symptomatic disease (abdominal pain, fever, fatigue) was associated with progressive lymphocytosis with an increase of > 50% over 1 month’s period (WBC 257.000/ mmc, L240.000/mmc).
On August the 1st, therapy with Ibrutinib had been started. As we expected, Lymphocytosis have trended steadily upwards to 375.000/mmc, followed by a gradual decreasing trend to 150.360/mmc in September with improvement of patient’s clinical condition (Figure 2).
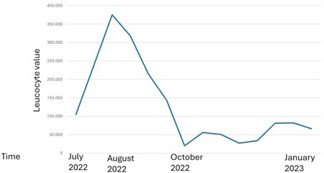
Figure 2: Trend of lymphocyte count before and after Ibrutinib discontinuation.
On October the 24th, patient presented an episode of nau-sea, vomiting and fatigue. Abdominal physical examination was negative. Sour vesicular murmur and basal crackling were de-tected at chest auscultation. Blood test, Chest-X-ray and test for Covid-19 were required and Ibrutinib was suspended until the receipt of the results in the suspicion of unset pneumonia.
On October the 26th the patient was admitted in ER for wors-ening of general malaise and fatigue. Chest’s CT scan revealed lobar pneumoniae and antimicrobial therapy with ceftriaxone and clarithromycin had started. Blood test results showed Hb 11.7 gr/dl, WBC 27.120/, lymphocyte 20.000/mmc, platelet count 86.000/mmc.
On October the 30th a second ER admission was required for acute abdominal pain. Abdominal CT scan revealed splenic artery’s pseudoaneurysm, large ruptured of subcapsular splenic hematoma > 50% and hemoperitoneum. (Figure 3) Splenic ar-tery embolization was performed. 24h after the onset CT con-trol showed an increasing splenic volume with 80% of ischemic rate. (Figure 4) Therefore, urgent Splenectomy and partial pan-createctomy were demanding.
Pathological examination showed a spleen size of 24 x 17 x 8 cm and a 9 cm capsular laceration. The cut surface showed a whitish micronodular aspect. Microscopic analysis of splenic and omentum sections points out a splenic infiltration of small lymphocytes with some nucleates elements with larger nuclei. Immunohistochemistry revealed the following phenotype: CD20+, CD23+, CD21-, CD5+. Ciclin D1 e SOX11 tested negative.
After surgical procedure peripheral blood examination showed Hb 7.9 gr/dl, WBC 66.750/mmc with lymphocyte 55.800/mmc, platelet count 317.000/mmc.
On December the 1st Ibrutinib had been reintroduced at full dosage after the completion of antibiotics and complete re-covery of the patient. After 1 month of ibrutinib, WBC count has been showing a stable trend around 60.000/mmc with im- provement in the patient’s clinical condition.
At 10 months of follow-up, patient is in good general con-dition carrying out his daily activities. Last blood test results showed improvement in hemoglobin value and stability of leu-kocyte value: Hb 15.6 gr/dl, WBC 67840/, lymphocyte 60560/ mmc, platelet count 335.000/mmc.
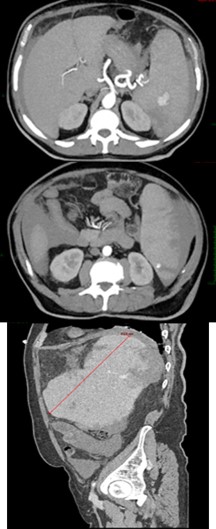
Figure 3: TC scan October 2022, pseudoaneurysm and hemoperitoneum previous embolization.
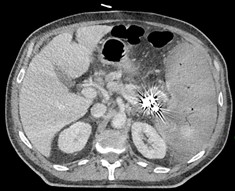
Figure 4: CT scan from November 2022 after embolization and prior splenectomy, showing splenomegaly with 80% ischemic rate.
We reported the case of an elderly Treatment Naïve (TN) pa-tient who discontinued Ibrutinib due to a pulmonary infection.
Many studies proved that toxicity, in particular infections, is the most common reason of Ibrutinib discontinuation [12-28].
CLLs is characterized by profound immune dysregulation, with enhanced susceptibility to infections. This could be ex-plained by CLL cells inhibiting antibody production by plasma cells and inducing neutropenia by bone marrow involvement, reducing the amount of peripheral mature B-cells antibody, and down regulating antigens expression of T and Natural-killer cells and more frequently to the effect of previous Immunochemo-therapy received [12-24].
Immunoglobulin A (IgA) is the predominant antibody iso-type in the mucosal immune system, which widely coats the gastrointestinal and respiratory tract. They have a fundamental role in protection against infections eliminating the pathogens with immune exclusion via nonspecific immunity. They repre-sent the first line of defence against respiratory viruses [17].
Sun C et al. observed, in a large cohort of patients during an extended 24 months follow-up, an increasing IgA levels within 6 months starting ibrutinib. IgG level remained stable in short-term decreasing with longer duration of drug. Moreover, they observed that ibrutinib decreased IgM levels in patient with clonal IgM, whereas increased IgM levels in patients without paraprotein [18].
Mato et al. recently demonstrate in a large cohort of pa-tients, both in and off clinical trials, that toxicity is the major reason of discontinuation both in the Relapsed/Refractory (R/R) and TN setting patients [13].
Differently, Susan O’Brien et al. shows how R/R patients dis-continued treatment most commonly because of disease pro-gression [14].
Contrary of what we observed in this case report, O’Brien et al. showed that grade ≥3 infections occurred less frequently among TN patients compared with R/R patients [15].
Similarly to what we described, in patients receiving ibruti-nib, the risk of infections was greatest during the first 3 months of therapy and decreased over time. Disease-related risk of infection seem to decrease following 6 months of treatment [16]. This could be related to several reasons, including early responses and disease, reduction of immunosuppressive T cells, extended time from last chemotherapy (in the case of R/R pa-tients), and the immune-modulating potential of ibrutinib [19].
Most of Clinical trials about ibrutinib reported that respirato-ry infections represent the 40% of all the infections. Streptococ-cus pneumoniae and Haemophilus influenzae are major causal agents for pneumonia and both are encapsulated bacteria, for which antibody response is crucial. 20 Over two decades, with extended use of ibrutinib, show an increasing incidence of in-vasive aspergillosis and other fungi, including Pnemocystis Ji-rovecii (PJ). PJ pneumonia in 5 % of cases could manifest with atypical clinical presentation, leading to delay in diagnosis [21].
During grade > 3 infections, temporary discontinuation of Ibrutinib is often recommended [22].
As Paul J. Hampela et al. overserved in his study 25% of pa-tient who temporarily discontinued Ibrutinib underwent to a progression of CLL disease or Richter’s transformation, manifest-ing worsening of symptoms and adenopathy, rising lymphocyte count and, as described by both Swetha Paduri and Porpaczy E. et al. in their case reports, it could also result in a rapid enlarge- ment and rupture of the spleen. Porpaczy E. et al hypotized that splenomegaly, before Ibrutinib is suspended, could represent a risk factor for this phenomenon [23-35]. Differently, Dutton et al. in his case report described a rapid drop of peripheral blood lymphocyte count followed by rapid increase of splenic size and his rupture, similarly to what we observed, hypothesizing that ibrutinib discontinuation could lead to systemic cytokine release and losing in lymphocyte proliferation and their hom-ing control to most of lymphoid tissues [26]. Moreover, they hypothesize that discontinuing Ibrutinib during a phase of sig-nificantly high lymphocyte count could represent a risk factor for splenic complications. Additionally, splenic rupture is also observed in other Hematologic disease like R/R Mantle cell lym-phoma in combined therapy ibrutinib and venetoclax [27].
Only 17% of splenic rupture cases have typical clinical mani-festation of acute abdomen hemoperitoneum [13]. Sometimes, elderly age, infection conditions and disease symptoms could mask clinical presentation determining an important diagnostic delay.
In order to prevent dangerous complications, especially dur-ing the first year of treatment, Ibrutinib discontinuation should be avoided and restricted only for necessary cases, like serious infections, especially when intravenous antibiotic or antifungal therapy is suggested.
We recommend to be careful in ibrutinib discontinuation in elderly patients who present lymphocytosis and splenomegaly.
For patient with severe splenomegaly, who necessitate Ibru-tinib discontinuation, we recommend frequent blood count monitoring, focusing on lymphocytosis, to exclude that sudden reduction is not an expected effect of the therapy but rather an indicator of splenic sequestration following drug discontinua-tion. Furthermore, it is useful to perform ultrasound monitoring every 2-3 months and a weekly physical examination or in case of pain in the upper left abdominal quadrant or at the apex of the contralateral shoulder. We suggest to educate the patients about the possible consequences without alarming them.
Moreover, in presence of signs of disease progression follow-ing the discontinuation of ibrutinib, it is always useful to per-form a disease reassessment. For example, in case of splenec-tomy, it is advisable to supplement the histological examination of the spleen with immunohistochemical analysis to exclude Richter transformation.
As we explained above, hypogammaglobulinemia is an infec-tion risk factor in particular for NT patients. We suggest that in this setting of patients monitoring Immunoglobulin serum lever could be a guide for IV immunoglobulin replacement prophy-laxis.
Over time, there has been growing recognition of the pos-sible consequences when discontinuing ibrutinib, along with valuable advice and warnings about exercising caution in such situations, including interruptions for medical procedures.