Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Isabelle Ried
Clinic for Cardiology, Pneumology and Internal Intensive Care Medicine, München Klinik Neuperlach, Germany.
Email: isabelle.ried@web.de
Received: Dec 30, 2025 Accepted: Jan 19, 2026 Published: Jan 26, 2026
Citation: Ried I, Segerer M, Hilge R, Guggemos W, Sack S, et al. Sepsis with thrombocytopenia and renal failure after a holiday at a lake in Eastern Europe. Ann Case Rep Med Images. 2026; 3(1): 1062.
Copyright: Ried I et al. © All rights are reserved
Leptospirosis is a zoonotic bacterial infection that is acquired through contact with infected animal urine, contaminated water, or soil. An infection may be missed due to late seroconversion.
A man in his 50s presented with fever, headache, nausea, and fatigue two days after returning from a trip to the Balkans. Initial laboratory findings showed thrombocytopenia, elevated inflammatory markers and impaired renal function. A strong clinical suspicion of leptospirosis was raised due to his exposure to contaminated water and rodents. Due to circulatory insufficiency, the patient had to be treated initially with catecholamines, and empirical therapy with piperacillin/ tazobactam was started. After clinical improvement, there was a second peak of fever and an increase in CRP on day 13 after admission. Subsequent serological tests after 17 days confirmed leptospirosis, so ceftriaxone was given. Within seven days of therapy, renal function and inflammatory markers improved significantly. The patient was discharged in good health.
Keywords: Difficulties in diagnosis; Sepsis; Thrombocytopenia; Renal failure; Leptospirosis.
Leptospirosis is transmitted through contact with infected animal urine or contaminated water. Initial symptoms can be nonspecific with high fever and muscle pain. In severe cases, patients may develop severe sepsis with thrombocytopenia, renal failure, meningitis, pulmonary haemorrhage, or liver failure with jaundice. Early diagnosis and antibiotic treatment are therefore crucial to prevent severe organ damage. However, the correct diagnosis may be missed due to late seroconversion. If the suspicion for leptospirosis is high, empiric antibiotic treatment in severe cases and repeated serologic testing is important. Leptospirosis is considered a “neglected infectious disease”, as it receives little attention, but it is a relevant global health threat [1].
A patient in his 50s was referred by his general practitioner to our internal medicine emergency department with reduced performance, headache, nausea, fever and aching limbs. The symptoms began shortly after a 10-day trip to the Balkans, during which he had travelled in a camper van with his son. During the trip, they bathed in several bodies of water, of which some were described as “contaminated”. They also stayed on a farm where numerous rodents were present. The patient sustained a small skin wound while doing woodwork on the farm. Symptoms appeared two days after returning home, while his son showed no symptoms. On admission, the patient was clinically alert and fully oriented with stable vital signs, blood pressure, 104/66 mmHg, heart rate, 80 beats/min, temperature, 37.1°C, respiratory rate, 14/min, saturation on room air, 95%. The clinical examination revealed no abnormal findings.
Investigations
The admission laboratory revealed a thrombocytopenia of 86/nl, an increase in inflammatory markers (CRP 385.6 mg/l, procalcitonin 23.86 µg/l) and renal retention parameters (creatinine 2.1 mg/dl, GFR 34 ml/min (Figure 1). A lactate of 3.3 mmol/l was measured in the initial blood gas analysis. Shortly there after, there was a progression of thrombocytopenia to 28/nl, and a rapid deterioration of the inflammation markers (CRP 426.2 mg/l, procalcitonin 122.16 µg/l) and renal retention parameters (creatinine 3.5 mg/dl, GFR 19 ml/min). In addition, D-dimer was elevated at 2.52 mg/l and troponin I at 244 ng/l. Additional laboratory findings (see Figures 1 and 2).
Serology for Hantavirus, Puumalavirus, SinNombre virus, Hantaanvirus, Dobravavirus, Seoulvirus, Borrelia, Rickettsia, HIV, hepatitis A/B/C, Mycoplasma, Legionella, Coxiella, were negative (Table 1).
We performed PCR tests for leptospirosis in EDTA blood and urine, both were negative. Quantiferon test was negative. PCR for Norovirus, Rotavirus, Adenovirus, Astrovirus, Sapovirus, Salmonella spp., Shigella / EIEC, Yersinia enterocolitica were negative. PCR for Adenovirus, Influenza A, Influenza B, RSV, SARSCoV-S, Parainfluenza, Hum. Rhinovirus, Metapneumovirus, they were all negative.
The initial imaging revealed no pathological findings. Radiographically, the cardiopulmonary status was unremarkable, with no evidence of an infiltrate. Sonography showed no evidence of an abdominal focus of infection. Echocardiography showed no vegetations or abscesses typical of endocarditis on any of the heart valves. The electrocardiogram was normal.
Differential diagnosis
According to the initial findings, the following suspected diagnoses were considered: Hantavirus infection, Lyme disease, or leptospirosis.
Hantavirus infection is a zoonosis caused by various types of hantaviruses. Transmission to humans occurs mainly through contact with the excreta of infected rodents, particularly via inhalation of virus-containing aerosol. The clinical symptoms vary depending on the virus type and geographical region. Asian and European hantavirus types can cause haemorrhagic fever with renal syndrome. This is characterized by flu-like symptoms with kidney involvement. Diagnosis is based on serological tests, in particular the detection of specific IgM and IgG antibodies by Enzyme-Linked Immunosorbent Assay (ELISA) and immunoblot or by direct immunofluorescence test. IgM antibodies are usually already detectable at the onset of clinical symptoms. The only clinical difference to leptospirosis is that Hantavirus infection does not affect liver function. Treatment is symptomatic, although haemodialysis or extracorporeal oxygenation may be necessary in severe cases. Preventive measures focus on avoiding contact with infected rodents and their excreta [2]. In our patient the serology for Hantavirus was negative.
Lyme disease, also known as Lyme borreliosis, is an infectious disease caused by bacteria of the genus Borrelia, which is mainly transmitted by tick bites. The disease is widespread worldwide, with a particular focus on the northern hemisphere. The symptoms of Lyme disease can progress in three stages: The early localised stage is often characterised by the characteristic erythema migrans, a spreading reddish skin lesion at the site of the tick bite. This was not detected in our patient but can be missed in some cases. In the early disseminated stage, flu-like symptoms, joint pain, and neurological complaints may occur.
The late stage can include chronic arthritis, neurological disorders and skin changes months to years after infection. Diagnosis is based on clinical symptoms, supported by serological tests such as ELISA and Western blot. Treatment is usually with antibiotics such as doxycycline, amoxicillin or ceftriaxone, with the duration and type of therapy depending on the stage of the disease. Prevention plays an important role and includes measures such as wearing protective clothing in tick areas, using insect repellent and removing ticks promptly after exposure [3]. Serology for Lyme disease in our patient was negative.
Leptospirosis is a worldwide bacterial zoonosis caused by spirochetes of the genus Leptospira. The disease is mainly transmitted through contact with urine from infected animals or contaminated water and soil. Risk factors include agricultural activities, sewage work, exposure to flooding and recreational activities in fresh water. The incubation period is 2-30 days, usually 5-14 days. Symptoms can range from mild and flu-like to severe (Weil’s disease), with possible complications such as kidney and liver failure, pulmonary haemorrhage, and meningitis. The most sensitive diagnosis involve direct detection of the pathogen using serological tests such as ELISA, PCR or culture. A major diagnostic challenge is that the initial serology and often also the cultures are usually negative. If there is clinical suspicion, it is therefore extremely important to repeat the serological tests. There are no standardised guidelines for the treatment of leptospirosis, but there is a consensus in favour of an early use of antibiotics such as doxycycline, penicillin or ceftriaxone, especially in severe cases, as well as supportive and symptomatic treatment. Preventive measures include wearing protective clothing in risk areas, strict hygiene measures and, in some countries, vaccination for high-risk groups [1,4,5]. In our patient serology on day 1 was negative, also PCR in the urine and EDTA blood. On day 17 serology for leptospirosis converted positive. Culture testing was not performed, because the specialised culture media for leptospirosis was not available in our laboratory.
Treatment
Due to circulatory insufficiency requiring catecholamines in the context of sepsis, which was accompanied by anuric renal failure and metabolic acidosis, after one day on the intermediate care ward, the patient was transferred to the internal medicine intensive care unit. Antibiotic treatment with piperacillin/ tazobactam led to an improvement of the infection parameters (Figures 1 & 2). Fluid replacement and low-dose catecholamine therapy quickly stabilised the patient and spontaneous diuresis was restored. Laboratory tests revealed pronounced thrombocytopenia, which occurs in up to 50% of patients with leptospirosis, correlates with renal failure, and is associated with a poorer prognosis [5]. In view of the patient’s contact with both contaminated water and rodents during his journey, we considered a Hantavirus infection or leptospirosis to be the most likely differential diagnoses. In consultation with our nephrology and infectiology colleagues, serological tests were carried out to further focus the search, but these did not reveal any evidence of an acute hantavirus infection, leptospirosis or Lyme disease. After six days of intensive care treatment, the patient was transferred to the normal ward. At day 13, there was an increase in inflammation markers and renal retention parameters. We still considered leptospirosis to be the most likely cause and started antibiotic treatment with ceftriaxone. The subsequent new serological examination showed a seroconversion of the Leptospira antibodies compared to the previous findings, which provided serological evidence of an acute infection. Antibiotic treatment with ceftriaxone was continued for a total of seven days (Figure 1).
Outcome and follow-up
The patient was discharged in good general condition with significantly improved renal function and almost normalised inflammatory markers. One year later, he is in good health, and his blood values are completely normalised.
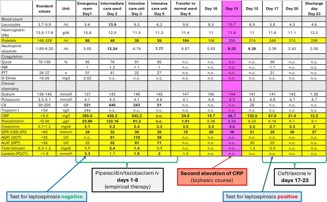
Figure 1
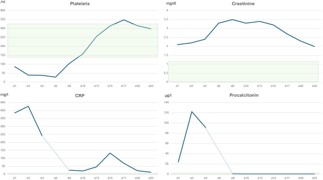
Figure 2
| Standard values | Unit | Intensive care unit | Normal ward (10 days later) | |
|---|---|---|---|---|
| Leptospira | ||||
| Leptospira IgG | Limit range 10-15 | U/ml | < 2 | 11,5 |
| Leptospira IgA | Limit range 12-20 | U/ml | 3,5 | >100 |
| Hantavirus | ||||
| Hanta-Virus IgG | Negative | Negative | ||
| Hanta-Virus IgM | Positive | Positive | ||
| Hanta-Virus IgM (Immunoblot) | Negative | Negative | ||
| Puumalavirus IgM | Negative | Negative | ||
| Sin-Nombrevirus IgM | Negative | Negative | ||
| Hantaanvirus IgM | Negative | Negative | ||
| Dobravavirus IgM | Negative | Negative | ||
| Seoulvirus IgM | Negative | Negative | ||
| Borrelia | ||||
| Borrelia IgG | <10 | AU/ml | 13 | n.c. |
| Borrelia IgM | <18 | AU/ml | <18 | n.c. |
| Borrelia IgG WB | Positive | n.c. | ||
| Borrelia IgM WB | Negative | n.c. | ||
| Rickettsia | ||||
| Rickettsia ricketsii IgG | <1:64 | Titer | <1:64 | n.c. |
| Rickettsia ricketsii IgM | <1:64 | Titer | <1:64 | n.c. |
| Rickettsia typhi IgG | <1:64 | Titer | <1:64 | n.c. |
| Rickettsia typhi IgM | <1:64 | Titer | <1:64 | n.c. |
| HIV-AG/AK CMIA | negative | negative | n.c. | |
| HBs-AG | negative | negative | n.c. |
In patients suffering from kidney failure, severe thrombocytopenia, and moderately elevated transaminase concentrations, acute leptospirosis should always be considered as part of the differential diagnosis, particularly considering a relevant travel or occupational history. Antibodies to Leptospira can take a week after illness onset to reach detectable levels [1]. It is therefore extremely important to start antibiotic therapy at an early stage in severe cases of leptospirosis with renal failure, thrombocytopenia, liver failure, or pulmonary haemorrhage if there is a high degree of clinical suspicion. The clinical presentation of leptospirosis is extremely varied, which contributes to a high number of unrecognised cases. It is under debate whether antibiotic therapy should be recommended in less severe cases [5]. Negative serological tests should be repeated after 7-10 days if there is clinical suspicion. The disease can lead to serious organ damage and is often characterised by a biphasic course. It is important to note that leptospirosis is classified as a notifiable disease in Germany and other countries and is also recognised as an occupational disease. These factors emphasise the importance of careful diagnosis and early detection of the disease, especially in patients with corresponding risk factors or occupational exposure [1,2,4].
Learning points/take home messages
1. Diagnosing leptospirosis can be challenging, as serological tests, culture, and even PCR are often negative in the early stages of the disease. Leptospirosis should nevertheless be considered in the differential diagnosis of patients presenting with renal and/or hepatic dysfunction, sepsis with thrombocytopenia, liver failure, meningitis, or pulmonary haemorrhage, particularly in the context of relevant travel history or occupational exposure. Initial negative serological tests for leptospirosis should be repeated after one week if clinical suspicion is high, and antibiotic treatment should not be delayed. PCR testing for leptospirosis can be done in urine, blood, or cerebrospinal fluid. Culture is difficult, requires several weeks of incubation, has low sensitivity, and requires specialised culture media [1].
2. The disease often follows a biphasic course and may result in severe organ damage. Due to its broad and nonspecific, clinical presentation, leptospirosis is frequently underrecognized or misdiagnosed.
3. Leptospirosis is a notifiable disease in Germany and is recognized as occupational disease. Our case report underscores the importance of early suspicion, thorough diagnostic evaluation, and timely treatment, especially in patients with risk factors or potential occupational exposure.
Conflict of interest: The authors declare no conflict of interest.
Patient consent: Written consent has been obtained from the patient concerned.