Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Lusanda Y Zongo
Department of General Surgery, Mthatha Regional Hospital, Mthatha, South Africa.
Email: lusanda.zongo@yahoo.com
Received: Dec 16, 2025 Accepted: Jan 05, 2026 Published: Jan 12, 2026
Citation: Zongo LY, Mamphiswana N, Nkomonye L, Choto C, Hoossen A, et al. Incidental diagnosis of superior vena cava syndrome secondary to lung mass in a patient presenting with haemorrhoids. Ann Case Rep Med Images. 2026; 3(1): 1060.
Copyright: Zongo LY et al. © All rights are reserved
Background: Haemorrhoids are common & often benign, but unrelated presentations can conceal serious disease.
Case: We report the case of a 56-year-old male who presented with a two-week history of painless rectal bleeding and perianal discomfort due to Grade II internal haemorrhoids. During evaluation, a thorough systemic examination revealed facial puffiness, distended neck veins, palpable axillary lymphadenopathy, and decreased air entry in the left upper lung zone—raising suspicion of an underlying intrathoracic pathology. Chest radiography showed left upper-zone opacity with mediastinal widening. Contrast CT revealed an 11×14×13 cm mediastinal mass with encasement of the aortic arch branches, occlusion of the left brachiocephalic vein, stenosis of the left pulmonary artery, and compression of the left main bronchus causing left upper-lobe collapse—features consistent with Superior Vena Cava Syndrome (SVCS) in a middle aged male with a history of chronic smoking and cannabis use. Axillary node histology demonstrated metastatic small-cell carcinoma (synaptophysin/chromogranin positive).
Management: Haemorrhoids were managed conservatively. SVCS was treated symptomatically with dexamethasone and urgent oncology referral for definitive chemoradiotherapy planning.
Conclusion: This case highlights the importance of comprehensive clinical assessment in patients presenting with common benign conditions. It reinforces the need for vigilance in identifying potentially life-threatening conditions that may initially present with unrelated or incidental complaints. Early recognition of SVCS enables timely oncologic management and prevention of complications.
Keywords: Superior Vena Cava Syndrome (SVCS); Small-Cell Lung Carcinoma (SCLC); Mediastinal mass; Incidental diagnosis; Haemorrhoids; Urgent oncology referral.
Haemorrhoids are dilated submucosal vascular cushions found within the anal canal, originating from a network of arteriovenous connective tissues that drain the superior and inferior hemorrhoidal veins [1].
Various factors can increase the risk of developing haemorrhoids, such as excessive straining during bowel movements or increased intra-abdominal pressure, which often results from constipation or prolonged sitting [1,2]. Haemorrhoids are classified by their anatomical location into three categories: internal (located above the dentate line), external (below the dentate line), or mixed types [1,2].
Internal haemorrhoids are innervated by visceral nerves, which makes them less sensitive to pain and irritation [1]. As a result, they can be asymptomatic or may present as painless perianal masses, itching, or small amounts of bright red blood during bowel movements, typically occurring at the end of defecation [1]. Both internal and external haemorrhoids are interconnected and drain into the internal pudendal veins, ultimately leading to the inferior vena cava. Internal haemorrhoids are further classified into four grades based on the extent of their prolapse:
− Grade I: Haemorrhoids are visible on anoscope and may bulge into the lumen, but do not prolapse below the dentate line [1].
− Grade II: Haemorrhoids prolapse out of the anal canal during defecation or straining but reduce spontaneously [1].
− Grade III: Haemorrhoids prolapse out of the anal canal with defecation or straining and require manual reduction [1].
− Grade IV: Haemorrhoids are irreducible and may become strangulated [1].
On the other hand, Superior Vena Cava Syndrome (SVCS) is characterized by venous congestion of the head, neck, and upper extremities due to impaired blood flow through the Superior Vena Cava (SVC) to the right atrium. SVCS can be divided into two main types: Malignant SVC syndrome, which accounts for more than 80% of cases, and Non-malignant SVC syndrome, which is often caused by thrombosis associated with an intravascular device, such as a dialysis catheter or pacemaker wire [3]. Typical clinical features of SVCS include facial swelling, upper limb oedema, and distended neck veins. Symptoms generally progress over weeks, although some patients may experience rapid deterioration that leads to an emergency situation [3]. In certain cases, SVCS may be incidentally discovered during investigations for unrelated medical issues [3,4].
A 56-year-old male presented to the surgical outpatient department with a two-week history of painless rectal bleeding, accompanied by perianal discomfort and occasional constipation. He was a known hypertensive, well-controlled on hydrochlorothiazide 12.5 mg once daily and amlodipine 5 mg once daily, with no other documented comorbidities. The patient has a long-standing history of tobacco and cannabis use, having initiated both at the age of 15. While he was unable to quantify his exact usage, he reported smoking fewer than 20 cigarettes per day and engaging in heavy, persistent cannabis use over the years. The patient denied any significant family history of malignancy or occupational exposure to carcinogens.
Systemic enquiry revealed recent onset of facial puffiness upon waking, hoarseness of voice, palpable lumps in the axillary regions, and unintentional weight loss. He denied any history of cough, chest pain, dyspnoea, or other respiratory symptoms.
On physical examination:
• General appearance: Facial plethora and puffiness, with prominent venous distension over the neck and anterior chest wall
• Vital signs: Within normal limits
• Lymphatic system: Bilateral, non-tender, mobile axillary lymphadenopathy
• Anorectal examination: Grade II internal haemorrhoids, with no external masses or signs of infection.
• Respiratory system: Reduced air entry in the left upper lung zone, with no added sounds
Investigations
Blood
| Category | Parameter | Results |
|---|---|---|
| Renal function & electrolyte | eGFR (CK-EPI) | 83 mL/min/1.73 m² |
| Creatinine | 89 µmol/L | |
| Urea | 2.9 mmol/L | |
| Inflammatory markers | CRP | 21 mg/L (High) |
| ESR | >130 mm/hr (High) | |
| Full blood count | Haemoglobin | 9.7 g/dL (Low) |
| MCV | 65.7 fL (Low) | |
| Platelets | 721x10¹/L (High) | |
| Neutrophils | 7.38x10¹/L (High) | |
| Lymphocytes | 1.17x10¹/L (Low) | |
| Iron studies | Serum Iron | 13 µmol/L (Normal) |
| Transferrin | 3.90 g/L (High) | |
| % Saturation | 13% (Low) | |
| Ferritin | 80 µg/L (Normal) | |
| Microbiology | MTB PCR | Negative |
Imaging: Chest radiograph
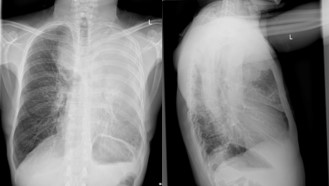
Figure 1: Chest radiograph: Left upper lobe opacity with widening of the mediastinum.
Imaging: CT chest, abdomen and pelvis with contrast
The CT report (dated 17 March 2025) reveals significant findings indicative of an aggressive mediastinal mass causing Superior Vena Cava Syndrome (SVCS).
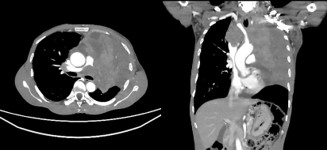
Figure 2: CT chest indicative of a mediastinal mass causing SVCS.
Key findings:
Large mediastinal mass:
• Size: 11×14×13 cm.
• Features: Necrotic areas, no calcifications or fat density.
• Suggests aggressive nature—possible malignancy.
1. Vascular and airway involvement:
• Encasement and compression of major vessels:
− Aortic arch and branches.
− Occlusion of the left brachiocephalic vein.
− Encasement of the left pulmonary artery → stenosis.
− Right brachiocephalic vein → reduced patency.
• Airway compression:
− Left main bronchus compression → left upper lobe collapse.
2. Pulmonary features:
• Right upper lobe: Emphysematous changes, bulla formation, and ground-glass opacities.
• No nodules, pleural effusion, or bone lesions noted.
3. Associated findings:
• Pericardial effusion.
• Abdominal organs normal except:
− Right kidney cyst.
− Distal rectal thickening with associated venous dilation.
− Para-aortic lymphadenopathy.
4. Comment:
• Mediastinal mass with vascular encasement and compression, with resultant superior vena cava syndrome.
Histopathology report from the axillary lymph node biopsy Summary of key findings:
Clinical background: Patient has a known lung mass as evidenced by imaging.
Specimen: Axillary lymph node measuring 30×25×20 mm, weighing 95g.
Histological features
o Effaced nodal architecture by tumour.
o Sheets of epithelial cells with nuclear moulding, apoptosis, mitotic activity.
o Cells with hyperchromatic nuclei and scant cytoplasm.
Final diagnosis
Metastatic small cell carcinoma, confirmed by immunohistochemistry:
Positive for MNF-116, Cam 5.2, synaptophysin, and chromogranin — all consistent with neuroendocrine differentiation, supporting small cell carcinoma.
Clinical implicationThis indicates that the patient’s axillary lymph node is involved by metastatic small cell lung carcinoma, an aggressive subtype with high metastatic potential.
Diagnosis
Grade II Internal haemorrhoids: Incidental superior vena cava syndrome due to compression by a mediastinal mass from left upper-lobe small-cell lung carcinoma SCLC
Management
Haemorrhoids: Managed conservatively with high-fibre diet, stool-softening regimen, sitz baths, and short course of topical haemorrhoidal agents.
SVCS due to SCLC: Initiated dexamethasone and analgesics for symptom relief; Urgent oncology referral for chemoradiotherapy; Smoking cessation counselling.
While SVCS is a recognised oncological emergency, it may present with subtle or atypical features, especially in early stages [3,5]. In this case, the patient’s presenting complaint was unrelated, and SVCS was only recognised on thorough systemic examination. Lung cancer remains the leading cause of SVCS [4,6]. Prompt identification is crucial to prevent complications such as cerebral oedema, airway compromise, and venous thrombosis [7,8].
From a public health perspective, while the association between tobacco use and lung cancer is well established, emerging evidence also highlights the significant risks linked to cannabis use. Notably, each joint-year of cannabis use (defined as smoking one joint per day for one year) is associated with an 8% increased risk of lung cancer [9]. Furthermore, smoking one cannabis joint per day has been shown to confer a comparable malignancy risk to that of smoking 20 cigarettes daily [9]. When used concurrently, tobacco and cannabis likely exert a compounded effect, further elevating the individual’s risk of developing lung cancer [9]. These findings underscore the importance of targeted health education for young people regarding the oncogenic potential of both substances.
This case underscores the necessity of a holistic approach to patient assessment. Even routine presentations such as haemorrhoids may harbour signs of more serious systemic pathology. Recognition of SVCS in early or atypical presentations is vital for timely intervention and better patient outcomes [3,4,10].
Limitation
Fibre-optic bronchoscopy and biopsy from the primary tumour, and colonoscopy were not performed due to logistical constraints.
Author contributions: Lusanda Y. Zongo: Conceptualization, original draft writing, and supervision. Northern Mamphiswana, Lithalethu Nkomonye: Case analysis, internal medicine insight and diagnostic input. Charles Choto, Amina Hoossen, Singleton Sandla, Ayabulela Sitshange, Siviwe Yako: Data collection, clinical coordination and literature review. Sijabulile Sosibo:
Critical revision and academic review.
Conflict of interest statement: Human Subjects: All participants provided informed consent for treatment and for the open-access publication of this case report, or such consent was waived in accordance with institutional policies.
Conflicts of interest:In accordance with the uniform disclosure requirements, the authors declare the following:
Payment/Services: No financial support or services were received from any external organization in relation to the submitted work.
Financial relationships: The authors report no financial relationships with any organizations that could be perceived to have an interest in the submitted work, either currently or within the past three years.
Other relationships: The authors declare no other relevant relationships or activities that could have influenced the content or outcomes of this study.
Acknowledgement: The authors would like to express sincere gratitude to the patient for granting consent to share their clinical information for educational and academic purposes. Appreciation is also extended to the nursing staff for their dedicated care, and invaluable support during the patient’s management, which contributed significantly to the successful documentation of this case.