Article Type: Case Report, Volume 3 Issue 1
*Corresponding author: Passa Roberto
Soft Tissue Sarcoma Surgery, University Hospital Campus BioMedico Foundation, Via Alvaro del Portillo 200, 00128 Rome, Italy.
Email: r.passa@policlinicocampus.it
Received: Dec 08, 2025 Accepted: Jan 02, 2026 Published: Jan 09, 2026
Citation: Lamattina S, Roberto P, Castagliuolo P, Pagnoni C, Angelucci M, et al. Giant recurrent retroperitoneal dedifferentiated liposarcoma: Case report and multidisciplinary therapeutic considerations. Ann Case Rep Med Images. 2026; 3(1): 1059.
Copyright: Roberto P et al. © All rights are reserved
Introduction: Retroperitoneal dedifferentiated liposarcoma represents a rare and aggressive mesenchymal neoplasm, frequently associated with a high propensity for local recurrence.
Case presentation: This report details the clinical course of a 56-year-old male patient presenting with an exceptionally large retroperitoneal liposarcoma, weighing approximately 40 kilograms. After an inadequate surgical resection, followed by experimental MDM2 inhibitor and high-dose chemotherapy, the clinical course was complicated by multiple local recurrences. The development of abdominal compressive symptoms led to the need for palliative surgery when tumor size was drastically increased.
Conclusion: This case underscores the complexity inherent in the palliative surgical management of advanced DDLPS and highlights the substantial therapeutic challenges, thereby emphasizing the role of a multidisciplinary approach.
Keywords: Dedifferentiated liposarcoma; Giant liposarcoma; Palliative surgery; Retroperitoneum.
Liposarcoma is one of the most common subtypes of retroperitoneal soft tissue sarcoma [1]. Dedifferentiated Liposarcoma (DDLPS) is a high-grade malignancy characterized by a significant risk of local recurrence and limited responsiveness to systemic therapies [2,3]. The anatomical complexity of the retroperitoneum hinders complete surgical resection, presenting substantial therapeutic challenges [4,5]. In this context, surgery remains the gold standard for achieving local disease control [6]. Radical surgical excision is frequently the only approach able to guarantee an improved long-term survival, particularly when it is performed in high-volume centers with access to multidisciplinary expertise [7]. Furthermore, in case of advanced or recurrent disease, surgery may also serve a palliative purpose, aimed at alleviating symptoms caused by mass effect or visceral compression. Retroperitoneal liposarcoma can reach significant dimensions. Thus, surgeons who approach this kind of tumors must be skilled on multivisceral resections. Often, liposarcoma size represents a further challenge.
We present the case of a 56-year-old male patient, former smoker, whose clinical history began in January 2023 with progressive abdominal distension and a palpable mass. Abdominal ultrasound and Computed Tomography (CT) scan revealed a large multilobulated lesion in the right retroperitoneum, displacing the small bowel, the right colon and the abdominal aorta. The patient initially underwent inadequate surgery in a nonspecialized centre in May 2023. The excision included only the mass. No other organs were resected. Final histopathological analysis revealed Grade 3 DDLPS. Surgical margins were positive for tumor infiltration. One month later, the patient was referred to our institute where he was enrolled in a clinical trial investigating the use of MDM2 inhibitor. He continued treatment until March 2024, when the follow-up showed progression disease. Oncologists switched therapy to high dose Ifosfamide. At the follow-up in June 2024, CT-scan showed a dimensional increase of the tumor, which extended to the inferior hepatic margin, involving the gallbladder and the uncinate-cephalic region of the pancreas. Chemotherapy changed into progressive lines: anthracycline followed by epirubicin and trabectedin. In January 2025, the patient presented to the emergency department with ascites and dyspnea caused by tumor compression. He was admitted to the oncology ward. During hospitalization, the patient formally expressed the possibility of undergoing palliative surgery. He was thoroughly informed about the potential benefits as well as the perioperative risks. After multidisciplinary discussion, palliative surgery was proposed, aware of the impossibility of reaching oncological radicality. Preoperative presentation of the patient is shown in (Figure 1). The preoperative CT-scan demonstrated an adipose mass occupying the middle and lower abdominal spaces, measuring approximately 40×31×50.5 cm. Preoperative CT-scan is shown in (Figure 2). The right hemidiaphragm was elevated beyond normal limits, causing hypoventilation. Furthermore, the hypochondrial organs were displaced cranially into the upper abdominal quadrants. The right colon and terminal ileum, together with several small bowel loops, were displaced anteriorly. The mass was inseparable from the external iliac artery and vein vascular bundle, exerting compressive effects on the vein up to the common iliac vein and the proximal third of the inferior vena cava. All these findings required meticulous dissection, which was essential to achieve complete tumor removal. On February 2025, we made surgical resection via xipho-pubic laparotomy followed by right transverse incision (Figure 3). Extensive adhesiolysis was performed to detach the mass from the abdominal wall on all sides. The lesion was then carefully separated from the ascending and transverse colon, both of which were displaced into the epigastrium. The mass was gradually mobilized in a proximal-to-distal direction, with dissection and isolation of the right ureter, which was encased by the tumor. The right common and external iliac arteries were preserved. As the right common iliac vein could not be safety separated, it was ligated and transected. This procedure was necessary and made possible by the presence of extensive collateral veins ensuring adequate venous drainage of the lower limb. Careful dissection was performed to detach the tumor from the bladder, followed by complete mobilization from the inguinal canal (Figure 4). During surgery, the patient received ten units of red blood cells concentrate, six units of plasma, and two platelet pools. The resected specimen consisted of a large lipomatous mass measuring 58×44×30 cm with a smooth external surface and satellite nodules (Figure 5). The tumor weight was incredibly around 40 kilograms. The patient was admitted to the Intensive Care Unit (ICU) for postoperative monitoring, where he remained for five days. His postoperative course was complicated by right external iliac artery thrombosis, which required bypass grafting. The patient was ultimately discharged on postoperative day 30 in good clinical conditions.

Figure 1: Preoperative presentation of the patient. Increased collateral venous circulation of the abdominal wall is shown. Side view (A), front view (B).

Figure 2: Preoperative CT-scan. The yellow arrow indicates DDLPS displacing visceral organs.
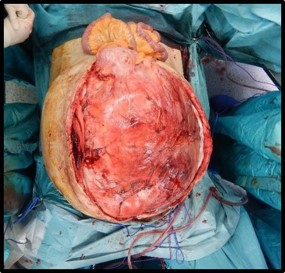
Figure 3: Intraoperative view of liposarcoma. Small bowel deplacement is shown.

Figure 4: Progressive mobilization of liposarcoma.
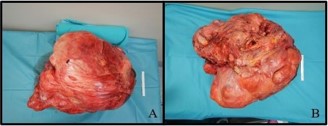
Figure 5: Macroscopic specimen. Front side (A). Back side (B).
DDLPS is characterized by insidious, asymptomatic growth to considerable size and a high propensity for local recurrence, even following macroscopically complete surgical excision. The present case exemplifies the typical clinical course of this challenging neoplasm, which is frequently marked by multiple recurrences, rapid disease progression and a significant impact on patient quality of life [8]. The palliative surgery was primarily aimed at alleviating compressive symptoms and preventing acute complications [9]. Despite advancements in systemic therapies, disease control remains largely transient and recurrence represent the principal cause of death [10]. The procedure was carried by a multidisciplinary team, including vascular surgeons whose expertise was critical in managing tumor involvement of the common iliac vein and addressing postoperative complications. Current literature underscores the importance of an integrated multidisciplinary approach in optimizing surgical outcomes and ensuring the safe management of retroperitoneal sarcomas [11]. Surgical treatment remains the gold standard on the management of DDLPS, as these tumors have poor response rates to chemotherapy or radiotherapy [12]. However, achieving negative margins does not eliminate the risk of local recurrence [7]. The potential benefit of organ resection to achieve negative margins must be carefully weighed against the morbidity associated with such procedures. As seen in other reported cases, palliative surgery was adopted as the only viable option given the rapid clinical deterioration and the risk of life threatening complications [13,14]. Future advances in systemic therapies, combined with early referral and multidisciplinary care, remain critical to improve prognosis of patients affected by DDLPS.
This case highlights the clinical and surgical challenges posed by giant retroperitoneal dedifferentiated liposarcoma. Despite its palliative intent, surgery proved effective in temporarily relieving compressive symptoms and improving the patient’s quality of life. The extreme tumor dimensions and vascular involvement required meticulous planning and a multidisciplinary approach, underscoring the main role of referral centres in managing such complex cases. Given the limited efficacy of systemic therapies and the high recurrence rate, individualized treatment and collaboration among surgical, oncological and radiological teams remain essential. To the best of our knowledge this is one of the largest retroperitoneal DDLPS surgically resected.