Article Type: Research Article, Volume 2 Issue 2
*Corresponding author: Song Wang
Department of Cardiovascular Surgery, Chongqing University Three Gorges Hospital, Chongqing, No. 165, Xincheng Road, Wanzhou District, Chongqing, 404000, China.
Email: wsily1987@163.com
Received: Nov 17, 2025 Accepted: Dec 17, 2025 Published: Dec 24, 2025
Citation: Su M, Duan H, Fang Z, Chang Y, Wang S, et al. The relationship between N-methyl-D-aspartate receptor and anxiety disorders accompanied by thyroid nodules. Ann Case Rep Med Images. 2025; 2(2): 1057.
Copyright: Wang S et al. © All rights are reserved
Objective: We previously found that N-Methyl-DAspartate Receptors (NMDAR) are likely associated with the pathogenesis of Anxiety Disorders (AD) and Thyroid Nodules (TN). This study aimed to investigate the predictive value of NMDAR and its subunits in the development of TN among patients with AD.
Methods: 397 patients with AD, with or without TN, hospitalized between October 2021 and March 2025 were recruited. Serum levels of NMDAR and its subunits (NR1, NR2A, and NR2B) were measured.
TN size and nature were assessed. Meanwhile, postoperative tissue specimens of Papillary Thyroid Carcinoma (PTC) from patients with and without AD were collected, and the expression differences of NMDAR subunits in PTC and its adjacent tissues were analyzed.
Results: Compared to patients with AD without TN (n=288), those with TN (n=109) were older, predominantly female, longer course of disease, and exhibited a higher level of NR2A subunit in serum. The NR2A subunit level was significantly correlated with the TN size. NR2A subunit levels, age, and female sex were significant predictors of TN occurrence in patients with AD, with an area under the curve of 0.837 (95% confidence interval: 0.792–0.882). Immunohistochemical analysis revealed significantly higher NR2A subunit expression but decreased NR2B subunit expression in PTC tissues compared to adjacent noncancerous tissues.
Conclusions: Elevated NR2A subunit levels, older age, and female sex are risk factors for TN development in patients with AD. The role of abnormal expression of NR2A and NR2B subunits in the progression of PTC warrant further investigation.
Keywords: N-methyl-D-aspartate receptor; Anxiety disorder; Thyroid nodule; Papillary thyroid carcinoma.
Anxiety Disorder (AD) is a prevalent mental health condition characterized by excessive anxiety, with a lifetime prevalence of approximately 34% [1], and the incidence rate has been on the rise in recent years [2]. It is reported that AD patients are often accompanied by Thyroid Nodules (TN), and the co-occurrence rate of the two is as high as 35.3% in China [3], which is significantly higher than the incidence rate of TN in the general population (20.4%) [4]. A retrospective study by Fischer et al. [5] indicated that AD often precedes the onset of thyroid diseases, suggesting an elevated risk of thyroid dysfunction or TN in patients with AD.
The incidence of thyroid cancer accounts for 7% to 15% of all TN cases [6], and it often induces or aggravates anxiety [7]. The athological types of thyroid cancer are diverse, with Papillary Thyroid Carcinoma (PTC) being the most common, accounting for over 85% of all thyroid cancers. It has been reported that 27% of PTC patients had anxiety or depression before surgery [8], and patients often changed the timing ofsurgical intervention due to anxiety [9]. However, the specific association and pathogenesis between AD and TN or PTC are unclear. Since these populations often have a relatively insidious onset and have inconspicuous clinical symptoms, they are often overlooked in the early stage of the disease, resulting in delayed clinical treatment and gradual deterioration of the condition. Therefore, studying the intrinsic relationship between AD and TN is of great significance.
N-Methyl-D-Aspartate Receptor (NMDAR) is a hetero-tetramer composed of three subunits: NR1, NR2 (A, B, C, and D), and NR3 (A and B). Among them, the NR1 and NR2 subunits are essential for the functional NMDAR, and the NR1 subunit is crucial for the assembly of the receptor, the transport of other subunits, and the functional activities of the receptor [10,11]. NMDAR is involved in various physiological and pathological processes in mammals and is primarily linked to emotional regulation and neurodegenerative diseases [12]. Emerging evidence suggests that NMDAR plays a role in tumorigenesis and progression [13,14]. We previously reported significantly higher expression levels of NMDAR and its subunits (NR1, NR2A, and NR2B) in the blood of patients with AD with TN compared to healthy controls, with NR2A subunit levels notably elevated in patients with AD with TN compared to those without TN [15]. While these findings suggest NMDAR’s involvement in AD and TN, the predictive value of NMDAR and its subunits for TN development in patients with AD has not been elucidated.
In this study, we hypothesized that NMDAR and its subunits have predictive value for the occurrence of TN among patients with AD and are related to the progression of PTC. We aimed to preliminarily verify this hypothesis through clinical research.
Study population and ethics
Patients admitted with a primary diagnosis of AD between October 2021 and March 2025 were enrolled in this cross-sectional study. Patients were divided into two groups based on the presence of TN: AD with TN (AD-TN group) and AD without TN (AD-NTN group). Meanwhile, postoperative PTC and its adjacent tissues of TN patients with or without AD were collected. All participants or their relatives provided written informed consent. This study was approved by the Ethics Committee of Three Gorges Hospital Affiliated with Chongqing University, with adherence to the principles of the Declaration of Helsinki throughout the research process.
Inclusion and exclusion criteria
The inclusion criteria were: (1) Patients diagnosed with AD per the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [16], with no prior TN history or unknown TN status, and a Hamilton Anxiety Scale (HAMA) score ≥7; (2) patients with TN meeting the 2015 American Thyroid Association (ATA) guidelines for adult thyroid nodules and differentiated thyroid cancer [17], with TN confirmed by ultrasonography and fine-needle aspiration (FNA) biopsy, including single or multiple nodules with at least one nodule ≥5 mm in maximum diameter [15], performed by experienced sonographers (with over 3 years of relevant experience); (3) patients with AD and TN meeting both aforementioned diagnostic criteria; and (4) patients within the age range of 18–65 years.
The exclusion criteria were: (1) Presence of neurological disorders; (2) Severe personality disorders or non-cooperation with the study; (3) Pregnancy or lactation; (4) Dependence on or abuse of psychoactive substances; (5) History of significant head trauma or organic brain disease; (6) Prior thyroid surgery or use of thyroid medications within the past month; and (7) Presence of tumors other than thyroid tumors.
Clinical data collection and scale scoring
Baseline data, including age, sex, Body Mass Index (BMI), medical history, and smoking/drinking history, were collected. Clinical assessments included thyroid hormone levels, anti-thyroid antibodies (including thyroglobulin antibodies and thyroid peroxidase antibodies), thyroid ultrasonography, HAMA scores, Hamilton Depression Scale (HAMD) scores, and surgical details. The HAMA and HAMA scores, comprising 14 items and 17 items respectively, with five response options scored from 0 (never) to 4 (extremely severe), was administered as previously described [18]. Based on total HAMA scores, AD severity was categorized as mild (7–13), moderate (14–23), or severe (≥24).
TN assessment and classification
TN were classified into categories I–V using the Thyroid Imaging Reporting and Data System (TI-RADS) [19]. Per the 2015 ATA guidelines, single or multiple TN with suspected malignancy (primarily TI-RADS ≥IV) or diameter >1 cm underwent FNA biopsy, with results reported using the Bethesda System (categories I–VI) [20].
TN were comprehensively classified based on Bethesda and TI-RADS as follows: Category A: Benign nodules (Bethesda II or TI-RADS I, II); Category B: Indeterminate nodules (Bethesda I, III, VI or TI-RADS III, VI); Category C: Suspicious malignant nodules (Bethesda V or TI-RADS V); Category D: Malignant nodules (Bethesda VI). In short, classification of TN primarily relied on Bethesda, supplemented by ultrasonography, TI-RADS, clinical expertise, and patient factors (e.g., family history of thyroid tumors). For surgically treated TN patients, the final classification was based on postoperative pathological findings.
Clinical sample collection and testing
Fasting peripheral blood samples were collected in the morning, and serum was separated by centrifugation and stored at -80°C. Serum levels of NMDAR and its subunits (including the NR1, NR2A, and NR2B) were quantified using enzyme-linked immunosorbent assay following the manufacturer’s instructions (Shanghai Ruifan Biotech). Each parameter was measured in duplicate, and the results were averaged. For patients with TN meeting the surgical criteria (especially those diagnosed with PTC by FNA) and consenting to surgery, traditional open surgery was performed, followed by routine paraffin sectioning and Immunohistochemical (IHC) analysis.
IHC experiment and image acquisition
Following our previously established protocol 15, IHC staining was performed on the postoperative PTC tissue specimens of patients with AD-TN to assess NR1, NR2A, and NR2B subunit expression. Key steps included deparaffinization, rehydration, endogenous enzyme inactivation, heat-mediated antigen retrieval, blocking, and incubation with primary antibodies (rabbit anti-human/mouse polyclonal antibodies, Hangzhou Huaan Biotech): anti-NR1 (1:100), anti-NR2A (1:75), and anti-NR2B (1:400). Sections were washed, incubated with secondary antibody (goat anti-rabbit IgG monoclonal antibody, Wuhan Boster Biotech), developed with 3, 3’-diaminobenzidine, counterstained with hematoxylin, dehydrated, cleared, and mounted. Images of NMDAR subunit-stained cells were captured using an Olympus DP74 microscope, and quantification was performed using ImageJ software and the IHC Toolbox, counting cells in five random fields at 200× magnification.
Statistical analyses
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 23.0. Categorical variables were expressed as frequencies or percentages, and continuous variables as means ± standard deviations. For normally distributed data, the independent samples t-test was used to compare between the two groups. One-way analysis of variance was performed for comparisons between multiple groups, followed by the least significant difference test or Dunnett’s test for post-hoc comparison of means of continuous variables between groups. Otherwise, distributions between different groups were compared using the Mann-Whitney U-test or Kruskal-Wallis H test for multiple independent samples. Group differences in categorical variables were compared using the χ² test. A p-value <0.05 was considered statistically significant.
Variables showing significant differences in the univariate analysis were included in a binary logistic regression model to assess their impact on TN development in patients with AD. Multivariate logistic regression analyzed the influence of NMDAR and its subunits on AD severity and TN classification. Multivariate linear regression examined the relationship between NMDAR subunit levels, HAMA scores, and TN size.
Baseline characteristics of patients with AD
A total of 400 patients with AD were screened, with 3 excluded (2 due to incomplete clinical data, and one due to prior thyroid surgery). Ultimately, 397 patients were included: 109 in the AD-TN group and 288 in the AD-NTN group. Compared to the AD-NTN group, the AD-TN group was older, and had a higher proportion of females and a longer course of disease (all p<0.05). There were no statistically significant differences in the remaining clinical indicators (all P>0.05; see Table 1 for details).
Clinical correlation between NMDAR with AD and TN
Compared to the AD-NTN group, the AD-TN group showed a significant higher expression of serum NR2A subunit (p<0.001; Table 2). In the binary logistic regression analysis, TN occurrence in patients with AD was the dependent variable, with clinical parameters showing significant group differences (age, sex, disease duration, and NR2A subunit level) as independent variables. Results indicated a positive correlation between TN occurrence and NR2A subunit levels, age, and female sex (B=0.049, 0.041, and 0.715; p were <0.001, 0.016, and 0.038, respectively; see Table 3). The combined predictive model yielded an Area Under the Curve (AUC) of 0.837 (95% CI: 0.792– 0.882), indicating a robust predictive value for TN development in patients with AD. Among them, the optimal cutoff value for the NR2A subunit was 119.9 pmol/L, with a sensitivity of 55.0% and a specificity of 91.7%.
To evaluate the impact of NMDAR and its subunits on AD and TN, multivariate ordinal logistic regression and linear regression analyses were conducted, with AD severity, TN classification, HAMA scores, and TN size as dependent variables and NMDAR and its subunits as independent variables. We observed a positive correlation between NR2B subunit levels and AD severity (B=0.007, p=0.003) and HAMA scores (B=0.023, p=0.002). NR2A subunit levels were positively correlated with TN size (B=0.031, p=0.006). However, no significant correlation was observed between NMDAR or its subunits and TN nature (comprehensive classification) (all p>0.05).
IHC analysis
A total of three patients with AD-TN were pathologically diagnosed with PTC and underwent radical resection of thyroid cancer. The results of IHC analysis showed that the NR1 subunit was widely expressed in PTC and its adjacent non-cancerous tissues, and there was no statistically significant difference between the two tissues (P>0.05).
NR2A subunit expression was significantly higher in PTC tissues compared to adjacent tissues (p=0.002). Interestingly, NR2B subunit expression was prevalent in adjacent tissues but nearly absent in PTC tissues (p=0.011; Figure 1).
| Clinical parameters | AD patient grouping | p-value | Clinical parameters |
|---|---|---|---|
| AD-TN group (n=109) | AD-NTN group (n=288) | ||
| Age (x±s), years | 55.6±8.7 | 53.2±9.5 | 0.021a |
| Female, N (%) | 90(82.6) | 202(70.1) | 0.012b |
| BMI (x±s), kg/m2 | 23.5±3.3 | 23.2±3.1 | 0.406a |
| Education level, N (%) | 0.078b | ||
| Primary or below | 58(53.2) | 117(40.6) | |
| Junior/Senior high school | 40(36.7) | 133(46.2) | |
| College or above | 11(10.1) | 38(13.2) | |
| Smoking history, N (%) | 4(3.7) | 10(3.5) | 1.000b |
| Drinking history, N (%) | 3(2.8) | 3(1.0) | 0.432b |
| Disease duration (x±s), months | 77.6±85.8 | 59.5±77.2 | 0.038a |
| HAMA score (x±s) | 15.3±6.5 | 15.4±5.8 | 0.923a |
| HAMD score (x±s) | 12.6±8.4 | 12.1±7.7 | 0.551a |
| Anxiety type, N (%) | 0.379b | ||
| GAD | 109(100.0) | 283(98.3) | |
| Panic attack | 0(0) | 5(1.7) | |
| Anxiety severity, N (%) | 0.994b | ||
| Mild | 45(41.3) | 119(41.3) | |
| Moderate | 53(48.6) | 141(49.0) | |
| Severe | 11(10.1) | 28(9.7) | |
| Comorbidities, N (%) | |||
| Hypertension | 26(23.9) | 55(19.1) | 0.294b |
| Diabetes | 7(6.4) | 27(9.4) | 0.348b |
| Coronary heart disease | 5(4.6) | 18(6.3) | 0.527b |
| Depressive disorder | 69(63.3) | 176(61.1) | 0.688b |
Notes: AD-TN group: patients with AD and TN; AD-NTN group: patients with AD without TN. X: mean; S: standard deviation; BMI: body mass index; N: number of cases; HAMA: Hamilton Anxiety Rating Scale (14-item printed version); HAMD: Hamilton Depression Scale (17-item printed version). GAD: generalized anxiety disorder. ᵃ: Independent samples t-test; ᵇ: χ² test.
| Clinical parameter | AD patient grouping | p-value | Clinical parameter |
|---|---|---|---|
| AD-TN group (n=162) | AD-NTN group (n=287) | ||
| NMDAR (x±s), pg/mL | 824.4±223.4 | 810.9±271.1 | 0.615a |
| NR1 (x±s), pg/mL | 166.0±60.2 | 176.5±67.8 | 0.135a |
| NR2A (x±s), pg/mL | 128.7±35.3 | 89.9±22.9 | <0.001a |
| NR2B (x±s), pg/mL | 159.5±45.2 | 160.8±51.4 | 0.804a |
| FT3 (x±s), pmol/L | 4.7±0.8 | 4.6±0.9 | 0.407a |
| FT4 (x±s), pmol/L | 15.1±3.3 | 15.5±3.5 | 0.398a |
| TSH (x±s), mIU/L | 2.1±2.6 | 2.5±2.8 | 0.153a |
| ATAb (+), N(%) | 13(11.9%) | 31(10.8%) | 0.742b |
Notes: NMDAR: N-methyl-D-aspartate receptor; NR: NMDAR subunit; FT3: free triiodothyronine; FT4: free thyroxine; TSH: thyroid-stimulating hormone; ATAb: anti-thyroid antibodies, including the thyroglobulin antibody (TGAb) and thyroid peroxidase antibody (TPOAb). ᵃ: Independent samples t-test; ᵇ: χ² test.
| Variable | B | OR Value | 95% CI | p-value |
|---|---|---|---|---|
| Age | 0.041 | 1.042 | 1.008 - 1.077 | 0.016 |
| Sex (female) | 0.715 | 2.043 | 1.040 - 4.012 | 0.038 |
| Disease duration | 0.003 | 1.003 | 0.999 - 1.006 | 0.147 |
| NR2A subunit | 0.049 | 1.050 | 1.039 - 1.061 | 0.000 |
Notes: B: regression coefficient; OR: odds ratio; CI: confidence interval.
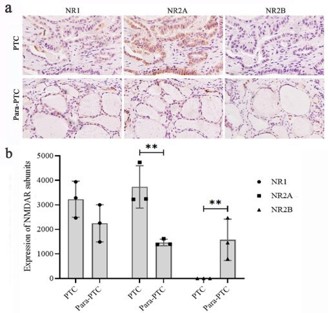
Figure 1: NMDAR subunit expression in postoperative PTC and ad
jacent tissues in patients with AD-TN (200x).
Notes: (a) Immunohistochemical staining; (b) Positive cell count for each NMDAR subunit. PTC, tissue samples of papillary thyroid carcinoma; Para-PTC: the adjacent tissues of papillary thyroid carcinoma. AD-TN: patients with AD and TN. *: P < 0.05; **: P < 0.01.
NMDAR and its subunits are extensively distributed in brain regions such as the prefrontal cortex, hippocampus, and hypothalamus, where they play a pivotal role in regulating emotions, including anxiety and depression [21,22]. The NR1 and NR2 subunits are essential for functional NMDAR, with abnormal NR2B subunit expression closely associated with AD [23,24]. We found a significant correlation between NR2B subunit levels and AD severity. These results further substantiate the role of NMDAR, particularly the NR2B subunit, in AD progression, potentially mediated by excitotoxicity resulting from NMDAR overexpression [25].
This study found that the incidence of TN among patients with AD was higher than the average incidence of TN among adults in China [4]. Previous studies have shown that abnormal expression of NMDAR can disrupt the structure of the thyroid gland and may be involved in the progression of thyroid tumors [26]. Mekkawy et al. [27] reported that high-dose monosodium glutamate (primarily sodium glutamate, which activates NMDAR) administration in rats led to significant damage to thyroid follicular epithelium and thyroid tissue degeneration. Similarly, our previous study [15] revealed that overexpression of NMDAR can affect the activity of the hypothalamic-pituitary thyroid axis. These results suggest that NMDAR overactivation exerts toxic effects on the thyroid.
In our study, serum NR2A subunit levels were significantly higher in patients with AD with TN compared to those without. IHC analysis revealed that, compared to the adjacent noncancerous tissues, high NR2A subunit expression in PTC tissues, whereas NR2B subunit expression was nearly absent in PTC tissues. Regression analyses confirmed a significant correlation between NR2A subunit levels and TN size, establishing NR2A as an importment risk factor for TN development in patients with AD. Previous studies have shown that elevated expression of NR2A subunit can promote the growth of thyroid cancer [28], and its mechanism may be to accelerate the cell cycle to promote tumor cell proliferation [29]. The reasons for the differential expression of NR2A and NR2B subunits in PTC tissues remain unclear, which may be related to gene methylation modifications or epigenetic inactivation [30,31], a hypothesis that requires further validation in future studies. Collectively, our findings indicate that aberrant NMDAR activity, particularly elevated NR2A subunit expressions, may be a critical contributor to TN development in patients with AD.
According to the ATA guidelines, most TN do not necessitate surgical intervention, underscoring the importance of comprehensive outpatient evaluation. Currently, ultrasonography using the TI-RADS classification and FNA with Bethesda classification serve as primary tools for preoperative assessment of TN malignancy [19,20]. Our study utilized Bethesda and TI-RADS classifications to comprehensively categorize TN malignancy. The results indicated no significant correlation between the comprehensive classification of TN and levels of NMDAR or its subunits (NR1, NR2A, and NR2B). These findings suggest that the beneness or malignancy of TN may not depend on serum levels of free NMDAR or its subunits. However, based on the AUC analysis of this study, the NR2A subunit may be an effective auxiliary tool for screening whether AD patients have TN due to its high specificity, thereby reducing misdiagnosis rates.
Interestingly, there was no statistically significant difference in HAMD scores and the proportion of depression between patients with AD with or without TN, indicating that the occurrence of TN may not be closely related to depression [32]. Our study found that patients with AD and TN were older and predominantly female compared to those without TN. Regression analysis confirmed a significant positive correlation between TN occurrence, age, and female sex. Further AUC analysis indicated that NR2A subunit levels, combined with age and female sex, provide robust predictive value for TN development in patients with AD, and the NR2A subunit also exhibited high specificity.
Numerous studies have established female sex as a risk factor for both AD and TN [33,34]. Our research group previously identified an association between TN occurrence in AD and age [15]. Clinically, heightened vigilance for TN risk is warranted in older female patients with AD. However, several limitations are worth elaborating. Firstly, this study is a single center clinical research and the distribution of patients is limited. Secondly, due to the limited number of thyroid tissue specimens available, this study did not investigate the correlation between the expression levels of NMDAR subunits in blood and thyroid tissue. Besides, the specific mechanisms of NMDAR subunits in TN and their effects on different pathological types of thyroid tumors remain unclear. These issues warrant further exploration in future researches.
This study confirmed the important role of NMDAR and its subunits in AD with TN through hematological and histological tests, providing valuable insights into the mechanisms underlying TN and thyroid tumor development. The roles of abnormal expression of NR2A and NR2B subunits in the progression of thyroid tumors deserve further study. The increased NR2A subunit, age, and female sex demonstrate good predictive value for TN occurrence in patients with AD, and the NR2A subunit may be used as an auxiliary tool for screening whether patients with AD have TN.
Author contributions: SML conceived and designed the study, collected clinical cases, managed funding, and was involved in drafting the manuscript. WS contributed to study design, data organization, immunohistochemical analysis, statistical analysis, and revised the manuscript. DHS, FZR, CY, ZJ, and WXT contributed to clinical case collection and specimen collection.
Acknowledgment: We would like to thank Duan Song and Xiang Shuang from the Department of Pathology at Chongqing University Three Gorges Hospital for their pathological guidance. Besides, we wish to acknowledge Editage for their professional English editing services.
Funding: This study was funded by the Chongqing Medical Scientific Research Project (Joint project of the Chongqing Health Commission and the Science and Technology Bureau, Grant No. 2024MSXM057) for their financial support.
Conflict of interest: The authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Data availability statement: Due to ethical restrictions, the data generated during this study cannot be made publicly available. Access to the data may be obtained from the corresponding author upon reasonable request.