Article Type: Review Article, Volume 2 Issue 2
*Corresponding author: Emmanuel Andres
Department of Internal Medicine, Hôpital de Hautepierre, University Hospital of Strasbourg, Strasbourg, France.
Email: emmanuel.andres@chru-strasbourg.fr
Received: Nov 25, 2025 Accepted: Dec 11, 2025 Published: Dec 18, 2025
Citation: Andres E, Jannot X, Terrade JE, Villalba NL. Definition of vitamin B12 deficiency: Concepts, biomarkers, grey zones, subclinical states, and diagnostic perspectives. Ann Case Rep Med Images. 2025; 2(2): 1055.
Copyright: Andres E et al. © All rights are reserved
Vitamin B12 deficiency, cobalamin deficiency, remains difficult to define because no single biomarker provides a reliable gold standard, and international consensus on diagnostic thresholds is lacking. Total serum vitamin B12 is widely used but lacks sensitivity and specificity, as it reflects both active and inactive fractions and is influenced by non–B12 factors. Holotranscobalamin improves early detection but suffers from limited availability and incomplete assay standardization. Functional biomarkers such as Methylmalonic Acid (MMA) and homocysteine offer greater sensitivity for detecting metabolic impairment, but their interpretation is influenced by renal function, folate status, and other confounding factors. These limitations generate a diagnostic “grey zone” in which borderline biochemical abnormalities coexist with variable clinical expression. Subclinical deficiency, defined by metabolic abnormalities without clinical signs, is common in elderly individuals, vegetarians, and patients with malabsorption or chronic medication exposure. Composite indices such as the combined indicator of B12 status (cB12) enhance diagnostic accuracy by integrating multiple markers, yet they remain insufficiently implemented. Current evidence supports a pragmatic, multi-marker approach that incorporates clinical context, metabolic testing, and risk assessment to define deficiency. Future progress requires assay standardization, outcome-based cut-offs, and validation of combined indicators across diverse populations.
Keywords: Vitamin B12 deficiency; Cobalamin; Methylmalonic acid; Holotranscobalamin; Homocysteine; biomarkers; Subclinical deficiency; Functional deficiency; Diagnostic grey zone; cB12 index; Assay standardization.
Vitamin B12 deficiency, cobalamin deficiency, is a common but often under-recognized condition that affects hematologic, neurologic, and systemic functions. The definition of vitamin B12 deficiency remains challenging because no universally accepted diagnostic standard exists, and interpretation relies on multiple imperfect biomarkers. The absence of a consensus threshold has produced heterogeneous clinical practices, inconsistent epidemiologic estimates, and uncertainty in patient management [1]. Many individuals present with biochemical abnormalities but lack classic symptoms, and many symptomatic patients exhibit borderline laboratory values. These diagnostic discrepancies reflect the complex physiology of cobalamin metabolism, assay variability, and the influence of comorbidities. Recent studies highlight the limitations of serum B12 alone and the need for complementary metabolic markers such as Methylmalonic Acid (MMA), homocysteine, and holotranscobalamin. The concept of subclinical deficiency further complicates interpretation, as metabolic impairment may precede clinical manifestations by months or years. Clinicians must therefore integrate biomarkers, clinical findings, and risk factors within a probabilistic framework. Understanding the strengths and weaknesses of available tests is essential for defining deficiency, managing at-risk populations, and guiding therapy.
This manuscript reviews current definitions, the biological basis of diagnostic uncertainty, and presents perspectives for improving the classification of cobalamin status.
Lack of an international diagnostic consensus
There is no global consensus on the definition of vitamin B12 deficiency. Thresholds for deficiency, insufficiency, and borderline status vary across laboratories, clinical guidelines, and research protocols. Some guidelines consider serum B12 <150 pmol/L (≈200 pg/mL) as diagnostic, while others propose higher cut-offs ranging from 221 to 300 pmol/L [2]. These ranges reflect differences in assay calibration, analytic performance, and population-based distributions. Variability also stems from heterogeneity in clinical endpoints used to determine deficiency, including hematologic parameters, metabolic markers, or neurologic symptoms. Several national societies recognize that serum B12 alone does not reliably reflect tissue status, but they diverge on whether to incorporate MMA, homocysteine, or holotranscobalamin as first-line or second-line tests [1,2]. This absence of standardized diagnostic criteria contrasts with other micronutrient deficiencies where consensus thresholds are widely accepted. Because no test provides definitive evidence of tissue depletion, diagnosis often relies on clinical judgment. This lack of consensus complicates clinical practice, hinders comparison across studies, and limits the development of unified clinical algorithms. Future efforts will require international collaboration, assay harmonization, and outcome-based definitions of deficiency.
Physiologic basis of biomarker variability
The physiological complexity of cobalamin metabolism contributes to diagnostic variability. Vitamin B12 circulates bound to two major proteins: transcobalamin, which delivers active cobalamin to cells, and haptocorrin, which binds the majority of circulating B12 but lacks metabolic function. Total serum B12 assays measure both fractions, creating discrepancies between circulating levels and intracellular availability. Cellular uptake further depends on receptor-mediated endocytosis, lysosomal processing, and cytosolic transport into enzyme systems [3]. Genetic differences in transcobalamin or methylmalonyl-CoA mutase can modify metabolic responses. Renal impairment alters MMA clearance, confounding interpretation. Liver disease increases serum B12 because of haptocorrin release. Cytokinemediated changes in haptocorrin during inflammation may mask true deficiency. These complex pathways explain why serum B12 may not reflect functional availability and why metabolic markers may rise despite apparently normal serum levels. Understanding these physiologic determinants helps clinicians appreciate the limits of available biomarkers and highlights the need for multi-marker approaches.
Total serum vitamin B12: Strengths and limitations
Total serum vitamin B12 remains the most frequently used first-line test because it is inexpensive, widely available, and well standardized relative to other biomarkers. Low serum B12 is strongly associated with clinical deficiency in many cohorts and provides a useful initial screen in high-risk patients [4]. However, serum B12 has important limitations. It reflects circulating concentrations rather than intracellular activity and includes inactive haptocorrin-bound B12. Serum levels fluctuate with diet, supplementation, liver function, inflammatory states, and binding protein abnormalities. False low values occur in pregnancy and folate deficiency, and false high values occur in hepatic disease, myeloproliferative disorders, renal failure, and solid tumors. Serum B12 shows poor correlation with MMA in many patients, especially in the elderly. Sensitivity for detecting early deficiency is limited, and specificity is modest. Despite these limitations, serum B12 remains useful when interpreted within a broader clinical algorithm. It provides a starting point rather than a definitive diagnosis [1,4].
Holotranscobalamin: The “Active B12” marker
Holotranscobalamin (holoTC), the fraction of vitamin B12 bound to transcobalamin, represents the biologically available pool capable of cellular uptake. HoloTC often decreases earlier than total B12 in the evolution of deficiency, making it a potentially sensitive marker for early or subclinical states [5]. Several studies demonstrate that low holoTC correlates with elevated MMA and homocysteine and improves diagnostic accuracy when combined with serum B12. HoloTC also shows better performance in pregnancy and in elderly patients. However, holoTC is not universally available, and assay standardization remains incomplete. Reference ranges vary between laboratories, and some clinicians remain unfamiliar with its interpretation. HoloTC can also be influenced by rare transcobalamin mutations, inflammation, and renal function. Despite these limitations, many experts consider holoTC a valuable addition to diagnostic algorithms, especially for borderline serum B12 values. Its ability to detect early tissue depletion makes it particularly relevant in preventive strategies.
Methylmalonic acid: A specific functional biomarker
Methylmalonic Acid (MMA) is a sensitive functional marker of intracellular vitamin B12 deficiency. MMA accumulates when the activity of methylmalonyl-CoA mutase decreases due to insufficient cobalamin. Elevated MMA strongly suggests impaired cellular B12 function, and it is considered one of the most specific biochemical indicators of deficiency [6]. MMA levels correlate with neurologic symptoms and respond quickly to supplementation, making it a useful monitoring marker. However, interpretation requires caution. Renal impairment increases MMA independently of B12 status, and age-related changes may shift reference intervals. Some rare inborn metabolic disorders also elevate MMA. Assays are more costly and less widely available than serum B12, limiting routine use. Nonetheless, MMA provides critical information for confirming deficiency when serum B12 or holoTC values are borderline [1,6]. Combining MMA with holoTC or serum B12 improves diagnostic discrimination.
Homocysteine: A sensitive but non-specific marker
Total homocysteine (tHcy) increases when methionine synthase function is impaired because of vitamin B12 or folate deficiency. Elevated tHcy is sensitive to both deficiencies and often rises earlier than hematologic changes. It is especially helpful in patients with dietary risks or mild symptoms. However, tHcy is not specific to B12 deficiency. Folate deficiency, vitamin B6 deficiency, renal impairment, thyroid disease, smoking, alcohol use, medications such as methotrexate, and genetic variants (MTHFR) all affect tHcy levels [7]. Because of these multiple confounders, tHcy is often used in combination with MMA to distinguish B12 from folate deficiency. tHcy can assist in establishing the diagnosis when interpreted alongside other biomarkers, but it should not be used in isolation. Its limited specificity restricts its utility in some clinical settings. Nevertheless, it remains a useful metabolic indicator within multi-marker approaches.
The grey zone: Borderline and indeterminate results
A major challenge in defining vitamin B12 deficiency is the diagnostic grey zone. Many patients present with serum B12 values in the borderline range (often defined as 150–300 pmol/L), and a substantial proportion of these individuals show metabolic abnormalities on MMA or tHcy testing [8]. Others remain asymptomatic with normal metabolic markers. This discordance illustrates the limited predictive value of single thresholds. Studies show that a sizeable proportion of elderly individuals fall within the grey zone because of age-related absorption decline, medication use, or comorbidities [2,8]. Determining which individuals require treatment remains controversial. Empiric supplementation is sometimes used, but evidence supporting clinical benefit in asymptomatic borderline cases is limited. The grey zone reflects the continuum of B12 status rather than a binary state. Clinicians must interpret borderline values by integrating symptoms, comorbidities, dietary intake, medication exposures, and confirmatory metabolic testing. Although multi-marker algorithms improve diagnostic resolution, they do not entirely remove residual uncertainty (Figure 1).
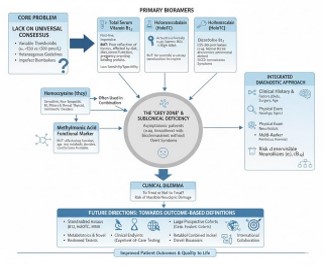
Figure 1: The diagnostic dillemba of vitaming vitamin B12 deficiency: An integrated biomaker and clinical approach.
Subclinical vitamin B12 deficiency
Subclinical vitamin B12 (cobalamin) deficiency (SCCD) is defined by biochemical abnormalities—most commonly low holoTC, mildly elevated MMA or homocysteine, or low-normal serum B12—without overt clinical signs [9]. SCCD is far more common than clinical deficiency and may precede symptoms by months or years. It is prevalent in older adults, vegetarians, patients taking metformin or proton pump inhibitors, and individuals with malabsorptive disorders. The clinical significance of SCCD remains debated. Some cohort studies suggest associations with cognitive decline, peripheral neuropathy, or frailty, but causality remains uncertain [9,10]. Randomized trials assessing treatment effects are limited and heterogeneous. SCCD likely represents a spectrum ranging from benign biochemical variation to evolving clinical deficiency. Early detection may prevent progression, but unnecessary supplementation should be avoided in low-risk asymptomatic individuals. More outcomebased research is needed to clarify the thresholds at which intervention is beneficial.
Subdeficiency, marginal status, and functional deficiency
Several authors distinguish between subdeficiency (marginal depletion), biochemical deficiency (low markers without clinical signs), and functional deficiency (metabolic impairment). These categories reflect the progressive physiological transitions from adequate stores to impaired cellular function and eventually to clinical manifestations [11]. Subdeficiency may be defined by low-normal serum B12 or holoTC without metabolic abnormalities. Biochemical deficiency is characterized by abnormal MMA or tHcy despite normal serum B12. Functional deficiency occur when metabolic impairment leads to symptoms. Differentiating these states remains challenging because symptom onset varies across individuals and depends on genetic predisposition, comorbidities, and lifestyle factors [9,11]. These distinctions underscore the inadequacy of fixed cut-offs based solely on serum values and the necessity of integrating metabolic and clinical data. The concept of functional deficiency is particularly important in neurologic disease, where irreversible damage can occur even without severe hematologic abnormalities.
Combined indicators: The cB12 and 4cB12 index
To overcome the limitations of single markers, composite indices such as the cB12 or four-marker combined indicator (4cB12) have been proposed. These models integrate serum B12, holoTC, MMA, and homocysteine into a single score that reflects the probability of deficiency [12]. This approach reduces discordance between markers and improves diagnostic accuracy. The cB12 index incorporates age adjustments and allows classification into categories ranging from “elevated status” to “deficiency.” Studies show that combined indicators outperform individual tests in predicting metabolic impairment. However, the use of such indices remains limited by availability of holoTC and MMA and by unfamiliarity among clinicians. Implementation also requires standardized reference intervals. Despite these challenges, the use of combined indicators marks an important move toward standardized definitions and more robust diagnostic approaches (Table 1). They offer a promising approach for research, for complex clinical cases, and for interpreting borderline results.
Clinical correlation: Signs, symptoms, and diagnostic implications
Clinical evaluation remains essential in defining vitamin B12 deficiency because biomarkers alone may be misleading. Classic signs include megaloblastic anemia, glossitis, peripheral neuropathy, cognitive impairment, gait disturbances, and psychiatric symptoms. Neurologic manifestations can occur without anemia, and hematologic changes may appear late. Some patients with severe biochemical abnormalities remain asymptomatic, whereas others with borderline markers present with significant neurologic dysfunction. Clinical history should explore dietary habits, medication use, gastrointestinal disorders, and risk factors for malabsorption. Physical examination may reveal subtle neurologic deficits that support diagnosis even when biomarkers are inconclusive. Treatment decisions often rely on combining clinical findings with biochemical evidence, especially when early neurologic involvement is suspected [13]. Clinical correlation helps distinguish true deficiency from false biochemical abnormalities due to comorbidities.
Populations at increased risk
Risk factors for vitamin B12 deficiency include advanced age, vegan or vegetarian diets, autoimmune gastritis, pernicious anemia, bariatric surgery, malabsorptive conditions, long-term use of metformin or proton pump inhibitors, chronic alcoholism, and certain genetic polymorphisms [14]. Elderly individuals frequently show borderline serum values and metabolic abnormalities due to gastric atrophy and reduced intrinsic factor production. Patients on metformin often exhibit reduced holoTC and elevated MMA. Bariatric surgery profoundly alters absorption and requires lifelong supplementation. Vegetarians and vegans may develop biochemical deficiency despite normal serum B12 if inactive analogs from plant sources are present.
Recognizing these populations is important because borderline biomarkers may require more aggressive interpretation [1,2]. High-risk individuals may benefit from earlier metabolic testing or empiric supplementation to prevent progression to symptomatic deficiency.
Diagnostic algorithms and clinical practice
Several diagnostic algorithms have been proposed to address uncertainty in defining B12 deficiency. Most start with serum B12 or holoTC as initial screening tests. Borderline or low results prompt confirmatory testing with MMA and sometimes tHcy, combined with evaluation of renal function and folate status. Clinical context guides interpretation at each step. Some algorithms recommend empiric supplementation when pre-test probability is high or when neurologic symptoms are present [14,15]. Others advocate for combined indicators in complex cases. While no algorithm is universally accepted, multi-marker strategies consistently improve accuracy over reliance on serum B12 alone. Algorithms that integrate risk factors, symptoms, and biomarkers may reduce misdiagnosis and unnecessary testing [1,14]. Further validation across diverse populations is needed to unify recommendations and inform evidence-based guidelines.
The problem of assay standardization
Assay variability remains a major obstacle in defining B12 deficiency. Differences in assay technology, calibration standards, reference intervals, and laboratory practices contribute to inconsistent results across institutions [1,15]. Serum B12 assays differ between immunoassay platforms. HoloTC lacks international standardization, and reference ranges vary widely. MMA measurement depends on gas or liquid chromatography methods, with substantial interlaboratory variation. These discrepancies hinder efforts to establish universal diagnostic cut-offs and complicate interpretation of multi-center studies. Standardization initiatives are underway but require coordinated action from clinical laboratories, regulatory agencies, and professional societies. Improved harmonization will enhance comparability of results, facilitate the use of combined indicators, and support development of consensus definitions [16].
Clinical outcomes and the need for evidence-based thresholds
Outcome-based definitions of deficiency are essential but underdeveloped. Most cut-offs are derived from population distributions rather than clinically meaningful endpoints [17]. Few trials assess whether treating biochemical abnormalities without symptoms prevents long-term complications. Observational data linking borderline markers with cognitive decline or neurologic symptoms are inconsistent. Randomized trials evaluating treatment in SCCD are limited and show variable outcomes. Outcome-based thresholds should ideally correlate with clinical improvement, reversal of metabolic abnormalities, or prevention of neurologic injury. Without such evidence, thresholds remain arbitrary and consensus elusive [16,17]. Future research must integrate clinical outcomes, biomarker changes, and patient-centered endpoints to refine definitions and guide treatment strategies.
Treatment implications of diagnostic uncertainty
Treatment decisions in borderline or subclinical states remain controversial. Oral cyanocobalamin is effective for most patients and carries minimal risk, making empiric therapy attractive. However, indiscriminate supplementation may mask underlying pathology such as pernicious anemia, cause inappropriate reassurance, or complicate diagnostic evaluation. On the other hand, delaying treatment in high-risk patients or those with neurologic symptoms may result in irreversible damage. Clinicians must balance the risks of over-treatment against the consequences of missed deficiency. Algorithms incorporating clinical judgment, risk factors, and metabolic markers can guide decision-making [18]. Treatment trials in SCCD populations are needed to clarify benefits and identify patient groups most likely to respond.
Perspectives for improved definitions
Future diagnostic strategies should aim for integrated, evidence-based definitions that incorporate biomarkers, clinical outcomes, and individualized risk assessment [19]. Standardized reference intervals for serum B12, holoTC, MMA, and tHcy are essential. Large prospective cohorts with clinical endpoints will help determine thresholds that predict meaningful outcomes. Emerging developments in metabolomics and functional biomarker research have the potential to provide more precise markers of intracellular deficiency. Combined indices such as cB12 should be refined and validated across diverse populations. Point-of-care testing may improve accessibility. Ultimately, consensus definitions will require collaboration among researchers, clinicians, laboratorians, and guideline committees.
| Biomarker | Physiological meaning | Strengths | Limitations / Confounders | Typical role in diagnosis |
|---|---|---|---|---|
| Serum vitamin B12 | Total circulating cobalamin (active + inactive fractions) | Widely available; inexpensive; good initial screen | Low sensitivity for early deficiency; elevated in liver disease, cancer, renal failure; reflects inactive haptocorrin fraction | First-line test; requires confirmation when borderline |
| Holotranscobalamin (holoTC) | Fraction of B12 available for cellular uptake | Early marker of deficiency; correlates well with MMA; improved sensitivity | Limited availability; assay variability; influenced by transcobalamin mutations and renal function | Second-line or comple- mentary marker; useful in borderline serum B12 |
| Methylmalonic acid (MMA) | Functional marker of intracellular B12 activity | High specificity for B12 deficiency; reflects metabolic impairment | Elevated in renal failure and some metabolic disorders; costlier; limited availability | Best confirmatory test for functional deficiency |
| Homocysteine (tHcy) | Marker of impaired methylation cycle | Sensitive early marker; useful when combined with MMA | Low specificity; influenced by folate/B6 deficiency, renal function, drugs, lifestyle | Supportive metabolic marker; never diagnostic alone |
| Combined indicator (cB12 / 4cB12) | Integrated score using B12, holoTC, MMA, ± homocysteine | Highest diagnostic accuracy; reduces discordance; probabilistic classification | Requires multiple assays; not widely implemented; needs standardization | Research and complex clinical cases; resolving indeterminate results |
Defining vitamin B12 deficiency remains complex due to limitations of available biomarkers, assay variability, and the spectrum from subclinical to overt clinical disease. The absence of a global consensus necessitates a pragmatic approach that combines serum markers, metabolic testing, clinical findings, and risk assessment. Multi-marker strategies improve accuracy and allow more nuanced interpretation of borderline results. Subclinical deficiency and the diagnostic grey zone remain areas of ongoing research, with important implications for prevention and treatment. Future progress will depend on assay standardization, outcome-based definitions, and validation of composite diagnostic indices. Until clearer consensus emerges, clinicians must integrate available evidence with clinical judgment to ensure timely diagnosis and appropriate management.
Conflict of interest: The authors declare no conflicts of interest.
Acknowledgements: The authors wish to thank all the clinicians and researchers of the CAREB12 group at the University Hospitals of Strasbourg for their invaluable contributions to patient care, data collection, and research support.