Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Elliot Brown
Division of Cardiology, The Valley Hospital, Paramus, NJ, USA.
Email: browel@valleyhealth.com
Received: Nov 08, 2025 Accepted: Dec 04, 2025 Published: Dec 11, 2025
Citation: Brown E, Imperatore G, Rahman-Kader S, Musat D, Jabagi H. Mitral valve replacement in severe mitral annular calcification: Managing periprosthetic leak and persistent symptoms. Ann Case Rep Med Images. 2025; 2(2): 1053.
Copyright: Brown E et al. © All rights are reserved
Background: Severe Mitral Annular Calcification (MAC) represents a rare but technically demanding condition that significantly increases operative risk during mitral valve surgery. Patients undergoing Mitral Valve Replacement (MVR) in this context are predisposed to structural, haemodynamic, and rhythm-related complications. Early identification of postoperative mechanical defects through multimodality imaging is crucial to improving outcomes.
Case presentation: A 70-year-old woman with moderate- to-severe mitral regurgitation, chronic kidney disease (stage 4), and persistent Atrial Fibrillation (AF) was referred for ablation but was found to have extensive MAC with central liquefaction necrosis. She underwent high-risk, chordal- sparing MVR using the “washer technique” with concomitant Maze procedure. Despite an initially successful operation, she developed recurrent AF and progressive dyspnoea.
Results: Transoesophageal Echocardiography (TEE) with 3D reconstruction demonstrated a circular perforation within the posterior felt patch placed between the mitral annulus and left atrial wall, resulting in a periprosthetic shunt from the left ventricle to the left atrium. Restoration of sinus rhythm through catheter ablation led to improved functional capacity and partial reduction of the regurgitant flow on follow-up echocardiography.
Conclusion: This case highlights the importance of advanced echocardiographic imaging in diagnosing rare postoperative complications after MVR in severe MAC. Mechanical patch perforation should be considered in the differential diagnosis of persistent symptoms following valve surgery, and a multidisciplinary approach remains essential for optimal management.
Keywords: Mitral annular calcification; Mitral valve replacement; Periprosthetic leak; Atrial fibrillation; Echocardiography.
Mitral Annular Calcification (MAC) is a chronic, degenerative process frequently encountered in elderly patients, often as- sociated with hypertension, atherosclerosis, and chronic renal disease [1,2]. While mild forms are common incidental findings on echocardiography, severe MAC significantly complicates mi- tral valve surgery due to the risk of atrioventricular disruption, paravalvular leak, and prosthesis instability [3,4]. This report describes a case of severe MAC requiring mitral valve replace- ment using the “washer technique”, complicated by a postoper- ative patch perforation producing periprosthetic regurgitation.
A woman in her seventies with a history of persistent atrial fibrillation, hypertension, hyperlipidaemia, and stage 4 chronic kidney disease was referred to our institution for catheter abla- tion after experiencing progressive exertional dyspnoea and re- duced exercise tolerance (New York Heart Association class III). On admission, her blood pressure was 130/63 mmHg, heart rate 107 beats per minute, respiratory rate 16 breaths per minute, and temperature 36.8°C. Jugular venous distension was absent, although a positive hepatojugular reflux was noted. Pulmonary auscultation was clear, and cardiac examination revealed an ir- regularly irregular tachycardic rhythm with a grade 2-3/6 systol- ic murmur best heard at the apex. No peripheral oedema was present. Because of her renal impairment, rhythm-control phar- macotherapy was limited, as she had previously not tolerated amiodarone. Therefore, a pulmonary vein isolation procedure was scheduled. The procedure was aborted intraoperatively af- ter intracardiac echocardiography revealed a large echodense mass in the left atrium. Subsequent multimodality imaging con- firmed extensive posterior Mitral Annular Calcification (MAC) with central liquefaction necrosis. Given the severity of her symptoms and underlying anatomy, the patient underwent a concomitant Maze procedure and high-risk, chordal-sparing Mitral Valve Replacement (MVR) using the “washer technique”. This method involves trigone-to-trigone felt patching along the posterior mitral annulus, interposed between the sewing ring of the prosthesis and the native annulus. Once the valve is se- cured, the remaining patch is sutured to the left atrial wall to reinforce the atrioventricular junction and prevent rupture.
Postoperative course
Although the operation was technically successful, the pa- tient continued to experience exertional dyspnoea, and her atrial fibrillation recurred. A repeat rhythm-control strategy was therefore considered, and a pre-ablation Transoesophageal Echocardiogram (TEE) was performed to reassess the integrity of the prosthetic valve and exclude left atrial appendage throm- bus (Figure 1). TEE demonstrated a well-seated mitral prosthesis with preserved leaflet motion and a crescent-shaped felt patch located posterior to the valve. Within the central portion of this patch, a circular fenestration measuring approximately 5 mm in diameter was identified, producing a high-velocity systolic jet directed from the left ventricle into the left atrium. No evidence of paravalvular leak, prosthetic dehiscence, or intrinsic valve dysfunction was observed. Three-dimensional TEE confirmed that the colour Doppler jet originated from a perforation within the posterior felt patch rather than true valvular regurgitation. Left ventricular systolic function was preserved, and there were no echocardiographic features suggestive of endocarditis or thrombus. Given these findings, a catheter ablation was per- formed to restore atrioventricular synchrony and reduce left atrial pressures, thereby minimising the shunt through the fen- estration. Following successful ablation, the patient reported marked symptomatic improvement (NYHA class II). Follow-up echocardiography demonstrated partial regression of the regur- gitant flow, decreasing from moderate–severe to moderate in severity. She has since remained in sinus rhythm and clinically stable on apixaban, metoprolol succinate, and diltiazem, with- out need for chronic diuretic therapy or further hospitalisation.
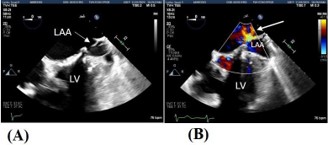
Figure 1: Transoesophageal Echocardiography images show no evidence of LAA thrombus (A), and an abnormal color doppler jet during systole (white arrow), which appears to be directed from the LAA toward the LA (B).
LAA: Left Atrial Appendage; LA: Left Atrium; LV: Left Ventricle.
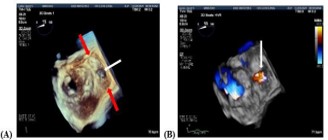
Figure 2: Three dimensional TEE images show the crescent shaped felt patch posterior to the mitral valve annulus shown by red arrows with central perforation shown by white arrow (A). Color doppler demonstrates systolic flow from the left ventricle to the left atrium through the fenestration in the felt patch as seen by the white arrow (B).
Severe MAC, prevalent in 2-3% of the general population and twice as common in women, reflects advanced fibro-calcific de- generation of the mitral annulus. Progression is accelerated by CKD, diabetes, smoking, and systemic atherosclerosis [1,5,6]. Surgical correction is technically demanding extensive calcium removal may risk atrioventricular disruption or left ventricular rupture, whereas incomplete debridement may impair pros- thetic seating [7]. The “washer technique”, described by Hus- sain et al. provides mechanical reinforcement by anchoring the prosthesis to a felt strip between the trigones [8]. While it preserves annular structure, it carries risk of patch perfora- tion, periprosthetic regurgitation, or atrial wall injury [8], as ob- served in this case. Persistent heart failure symptoms after MVR in severe MAC should prompt evaluation for paravalvular leak, valve dehiscence, endocarditis, patch or annular disruption, and arrhythmic dysfunction [9,10]. In this patient, TEE with 3D reconstruction was essential in differentiating true prosthetic regurgitation from a localized periprosthetic shunt (Figure 2). Color Doppler allowed accurate visualization of flow direction, confirming a ventricular-to-atrial leak [11,12]. Given the pa- tient’s comorbidities and stable hemodynamics, a conservative approach was adopted. Rhythm restoration via AF ablation effectively reduced regurgitant flow by re-establishing atrioven- tricular synchrony and lowering left atrial pressure. Close im- aging follow-up every 3-6 months was advised, with surgical revision reserved for progressive leak or recurrent heart failure.
Mitral valve replacement in the setting of severe annular calcification remains one of the most challenging procedures in cardiac surgery. Postoperative dyspnoea in such patients should raise suspicion for structural complications beyond typical valve dysfunction. Three-dimensional TEE plays a pivotal role in di- agnosis and follow-up, while individualized multidisciplinary management - integrating cardiology, cardiac surgery, and elec- trophysiology - is key to optimizing outcomes.
Learning points
• Severe MAC markedly increases the complexity and risk of mitral valve replacement.
• Patch perforation following the “washer technique” is a rare but important cause of periprosthetic regurgitation.
• 3D TEE provides superior visualization of postoperative anatomy and should be the first-line modality for unexplained symptoms.
• Rhythm control in patients with recurrent AF can mitigate regurgitant flow and improve functional status.
• Long-term multidisciplinary follow-up is crucial for early detection of mechanical and arrhythmic complications.
Patient perspective
“After my mitral valve surgery, I initially felt better but soon became short of breath again when my atrial fibrillation re- turned. The doctors discovered a small hole near the valve patch, and after a second ablation, my energy improved. I’m grateful to have a coordinated team monitoring my valve regu- larly - it gives me confidence and peace of mind.”
Consent for publication: Written informed consent was obtained from the patient for publication of this case report.
Conflict of interest: The authors declare no conflict of interest.
Funding: This research received no external funding.
Acknowledgement: The authors thank the cardiology and cardiac surgery teams at The Valley Hospital for their collaboration in patient management.