Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Giovanni Del Fabro
Department of Infectious Diseases, ASFO “Santa Maria Degli Angeli” Hospital of Pordenone, Pordenone, Italy.
Email: giovanni.delfabro@asfo.sanita.fvg.it
Received: Oct 02, 2025 Accepted: Nov 19, 2025 Published: Nov 26, 2025
Citation: Fabro GD, Chimienti E, Lleshi A, Stanzione B, Spina M, et al. Not always in pairs! A case of unilateral Pneumocystis pneumonia. Ann Case Rep Med Images. 2025; 2(2): 1052.
Copyright: Fabro GD et al. © All rights are reserved
Background: Pneumocystis Jirovecii Pneumonia (PJP) is an opportunistic infection increasingly observed in non-HIV immunocompromised patients, with mortality rates up to 50%. The typical radiological pattern is bilateral interstitial pneumonia with diffuse ground-glass opacities. However, atypical presentations, including unilateral disease, can occur and may delay diagnosis.
Case presentation: We describe a 67-year-old HIVnegative man with diffuse large B-cell lymphoma on chemotherapy. Shortly after recovery from chemotherapyinduced neutropenia, he presented with fever and progressive respiratory failure unresponsive to broadspectrum antibiotics. Laboratory tests showed elevated inflammatory markers and severe lymphopenia. Chest CT revealed interstitial ground-glass opacities confined to the right lung. Despite the atypical unilateral involvement, PJP was suspected due to the patient’s risk factors. Empirical therapy with cotrimoxazole and methylprednisolone was initiated. Diagnosis was later confirmed by positive serum β-D-glucan and Bronchoalveolar Lavage (BAL), which detected >14,000 copies of P. jirovecii. The patient improved progressively and achieved full recovery. A follow-up CT one month later showed resolution of the right-sided infiltrates.
Conclusion: Atypical unilateral disease should not rule out the diagnosis of PJP. Maintaining a high index of suspicion in at-risk patients, even with unusual radiological findings, is critical. Early initiation of empirical therapy is essential, as prompt treatment significantly reduces mortality.
Keywords:Pneumocystis jirovecii pneumonia; Unilateral pneumonia; Hematologic malignancy.
Pneumocystis Jirovecii Pneumonia (PJP) is an opportunistic infection increasingly reported in non-HIV patients, with mortality rates up to 50%. At-risk groups include patients with hematologic malignancies, chronic lung disease, and those receiving immunosuppressive therapies (e.g., high-dose steroids, cyclosporine, tyrosine kinase inhibitors) [1,2].
Early treatment is crucial for survival, but diagnosis requires a high index of suspicion. PJP usually presents with progressive dyspnea, fever, and cough. The typical radiological finding is bilateral interstitial pneumonia with diffuse ground-glass opacities, more pronounced in apical and perihilar regions [1]. Atypical forms, such as unilateral disease or lobar consolidation, are rarely described and can be misleading [3]. We present here the case of a patient with Pneumocystis pneumonia showing unilateral radiological involvement. Written informed consent was obtained from the patient prior to publication.
A 67-year-old HIV-negative man with diffuse large B-cell lymphoma was receiving R-CHOP chemotherapy (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone). During chemotherapy-induced neutropenia, he developed Enterococcus faecalis bacteremia. After targeted antibiotic therapy and resolution of neutropenia, he developed recurrent fever and progressive respiratory failure. Empirical treatment with piperacillin/tazobactam was ineffective.
Blood tests showed elevated inflammatory markers (CRP 4 mg/dL, PCT 0.38 µg/L) and severe lymphopenia (260/µL). Chest CT revealed unilateral interstitial ground-glass opacities confined to the right lung (Figure 1). Given the patient’s risk factors and presentation, PJP was suspected despite the atypical radiology.
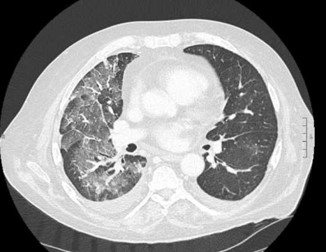
Figure 1: First axial CT-scan of the chest shows diffuse ground-glass opacities in the right lung parenchyma, associated with a basal pleural effusion.
Empirical cotrimoxazole and methylprednisolone were started, and piperacillin/tazobactam were stopped. One week later, the diagnosis was confirmed by positive serum β-D-glucan and BAL analysis (>14,000 P. jirovecii copies). Respiratory function worsened briefly in the first 48-72 hours, then improved progressively. The patient achieved complete recovery. A follow-up CT one month later showed near-complete resolution of rightsided infiltrates (Figure 2).

Figure 2: First axial CT-scan of the chest shows diffuse ground-glass opacities in the right lung parenchyma, associated with a basal pleural effusion.
Pneumocystis Jirovecii Pneumonia (PJP) typically presents with bilateral diffuse Ground-Glass Opacities (GGO), often with apical or perihilar predominance. This radiological pattern is highly suggestive in the appropriate clinical setting and remains the most frequent presentation in both HIV-positive and nonHIV immunocompromised patients [4].
However, several atypical imaging patterns have been described, especially in non-HIV populations, where PJP often progresses more rapidly and presents with greater radiologic heterogeneity. These include unilateral involvement, lobar or segmental distribution, patchy consolidations, nodular opacities, cavitary lesions, and even pneumothorax or cyst formation [5-7]. Such atypical features may mimic alternative diagnoses, including bacterial pneumonia, viral infections, organizing pneumonia, or drug-induced lung injury, often delaying the correct diagnosis.
Unilateral PJP, as observed in our patient, is particularly uncommon. Case series suggest that it accounts for fewer than 5-10% of reported presentations [7]. The underlying mechanisms are not fully understood. Hypotheses include localized variations in host immune response, uneven distribution of pathogen burden, or concurrent conditions influencing regional susceptibility of lung parenchyma [5].
Recognition of these atypical forms is essential, especially in non-HIV immunocompromised patients, where clinical suspicion may already be lower than in HIV-infected individuals. A high index of suspicion should therefore be maintained in patients with compatible risk factors (hematologic malignancy, lymphopenia, immunosuppressive therapy), even when imaging findings deviate from the classic pattern. In such cases, empirical initiation of anti-PJP therapy while awaiting confirmatory diagnostics can be lifesaving.
PJP usually presents with bilateral pneumonia. However, unilateral involvement does not exclude the diagnosis. Clinicians must maintain suspicion in at-risk patients, even with atypical radiology. Empirical therapy should be started when suspicion is high, as early treatment reduces mortality [2].