Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Xiao Long
The Xiaolifeidao Medical Cosmetology Hospital, Guiyang, Guizhou, 550081, China.
Email: 25481455@qq.com
Received: Oct 16, 2025 Accepted: Nov 10, 2025 Published: Nov 17, 2025
Citation: Long X. Botulinum toxin type a treatment for Meige syndrome - A case of blepharospasm combined with oromandibular dystonia and literature review. Ann Case Rep Med Images. 2025; 2(2): 1049.
Copyright: Long X et al. © All rights are reserved
Background: Meige Syndrome (MS) is characterized by blepharospasm and oromandibular dystonia that are often refractory to oral medications.
Case presentation: A 59-year-old woman with persistent symptoms despite polypharmacy received intramuscular botulinum toxin type A (BTX-A, Prosigne®) from the Lanzhou Institute of Biological Products. Individualized injection sites and doses were selected according to clinical severity. Post-injection facial spasms markedly diminished, nocturnal headaches resolved, no adverse events were noted, and normal social and feeding functions were restored.
Conclusion: BTX-A is a safe, effective treatment for MS, rapidly relieving dystonia and improving quality of life; ultrasound guidance may further enhance accuracy and safety.
Keywords: Meige syndrome; Blepharospasm; Oromandibular dystonia; Botulinum toxin.
Meige Syndrome (MS) is a rare neurological disease belonging to the category of segmental dystonia. It is also known as eyelid-mandibular dystonia syndrome and primarily causes various forms of dystonia in the eyelid, facial muscles, mandible, and neck muscles. It usually onset in adulthood and is more common in the elderly. Bilateral blepharospasm and oromandibular dystonia are the two main clinical features of this disease [1]. Blepharospasm is typically the first symptom and can progress to other cranial nerves and extracranial muscles as the disease advances [2]. The disease was first described by French neurologist Henry Meige in 1910 and was named after him. The clinical manifestations include eye discomfort, increased blinking, excessive eye opening, and eye closure symptoms, along with involuntary mouth opening, closing, pouting, abnormal lip twitching, teeth grinding, tongue protrusion, tongue biting, etc. These symptoms often worsen during speech and eating, resulting in a bizarre expression that can severely affect the patient’s eating, speech function, appearance, and self-esteem [3]. In clinical practice, the diagnosis and treatment system of plastic surgery has relatively limited exposure to MS, leading to a lack of understanding and clinical experience regarding this condition. Recently, we successfully improved the symptoms of a patient with blepharospasm and oromandibular dystonia type MS using an individualized BTX-A injection plan in our outpatient department. This report provides a systematic analysis of the case characteristics, dosage allocation strategy, and dynamic follow-up results.
A 59-year-old female patient presented with involuntary eye squeezing, frowning, and twitching of the eyelids without any identifiable cause 16 years ago. The twitching episodes were intermittent and increased in frequency with age. She also experienced involuntary pouting, grimacing during speech, and nighttime headaches that were uncontrollable. She had repeatedly visited the neurology department of other hospitals for systematic diagnosis and treatment, including medication, traditional Chinese medicine physiotherapy, and acupuncture. Although her symptoms improved somewhat with treatment, they were not effectively controlled, especially during speaking and eating activities. She discontinued the medication on her own. After discontinuation, the symptoms persisted, and despite seeking medical help from various sources, no significant improvement was achieved. In June of last year, the patient visited our hospital for treatment of facial spots and wrinkles. During the consultation, it was observed that the patient had severe static wrinkles around the eyes and mouth. She frequently raised her eyebrows, squeezed her eyes, and had a forced smile when speaking, resulting in a peculiar expression. After taking a detailed medical history and communicating thoroughly, it was recommended that the patient undergo BTX-A injections in the affected facial areas, to which she agreed.
Physical examination at the time of treatment revealed symmetric forehead lines with moderate wrinkles, mild to moderate glabellar and medial canthal wrinkles, severe transverse wrinkles at the nasal root, and lateral canthal fish-tail wrinkles. Mild vertical lip lines were present in the upper and lower lip white areas. When closing her eyes, the patient exhibited frequent twitching of the bilateral eyelids and eyebrows, along with continuous nose wrinkling. The wrinkles at the medial and lateral canthi of the upper and lower eyelids and the transverse nasal root wrinkles were deepened. Severe oblique wrinkles appeared in the middle of the nasal dorsum. The lips frequently contracted involuntarily and pursed, with deepened vertical lip lines (Figure 1). When opening her eyes and speaking, the frontalis and glabellar muscles contracted involuntarily, causing the eyebrows to rise and deepen the forehead lines. The upper eyelids were passively elevated, leading to widened eye fissures and overexposure of the eyeballs, resulting in a “staring” appearance. This was accompanied by dilated nares, involuntary lip twitching, a forced smile-like mouth opening, excessive elevation of the upper lip, complete exposure of the gums, and the formation of a severe “gummy smile [4].” The nasolabial folds were deepened, particularly on the left side, with a slight leftward deviation of the mouth corner (Figure 2).
Treatment plan
Due to the lack of comparative studies on this condition and the diversity of clinical manifestations, the treatment plan was primarily based on the author’s clinical experience, as well as the location and severity of muscle spasms in the patient. Preoperative imaging data were routinely collected, and informed consent was signed. The BTX-A used for injection (Prosigne®) was produced by the Lanzhou Institute of Biological Products in China. The dose was 100 U per vial, diluted with 2.0 ml of 0.9% normal saline (50 U/ml), using a 1 ml syringe and a 4 mm (34 G) injection needle (Figure 7 & Table 1). Seven months after the initial injection, the patient returned for a follow-up visit and received another injection treatment using the same BTX-A product at a dose of 50 U per vial, diluted with 1.0 ml of 0.9% normal saline (50 U/ml), using a 1 ml syringe and a 4 mm (34 G) injection needle. Three weeks after the second injection, the patient returned for a supplementary injection.
One week after the initial injection, the patient’s facial symptoms improved significantly, although there was mild facial rigidity (Figure 3). She experienced mild skin tightness and discomfort in the forehead and periorbital areas. By onemonth post-injection, the treatment was fully effective, with the resolution of nighttime headaches and adverse reactions. Within three months after the initial injection, symptoms such as eyebrow raising, eye squeezing, mouth pursing, twitching, and headaches did not recur. The patient’s expression appeared natural, allowing for normal social interaction and eating, and she was essentially free from the disease’s impact. Four months later, the patient returned for a follow-up visit. Her facial expression was natural, and forehead lines were visible. When speaking, there was mild contraction of the frontalis muscle and slight elevation of the eyebrows. The eyes blinked frequently without twitching, and the mouth pursed frequently with mild twitching of the mouth corners. The patient’s mouth opening and smiling appeared natural, with no excessive elevation of the upper lip, no lip deviation, and no “forced smile” or “gummy smile” expressions (Figure 4).

Figure 1: The state with eyes closed during the first medical visit.
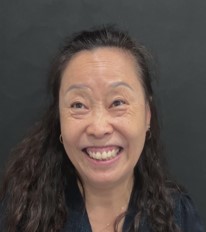
Figure 2: The state when speaking with eyes open during the first medical visit.

Figure 3: 7 days after the first botulinum toxin injection treatment.

Figure 4: 4 months after the first botulinum toxin inection treatment.

Figure 5: At the follow-up visit 7 months after the first injection, the state with eyes closed.
Seven months after the initial injection, the patient returned for another follow-up. Physical examination revealed improvements in forehead lines, periorbital wrinkles, and nasal dorsum wrinkles compared to the initial visit. When closing her eyes, there were frequent mild twitching of the bilateral eyelids without nose wrinkling (Figure 5). The lips occasionally exhibited mild involuntary contraction and pursing. The patient displayed involuntary lip twitching, a forced smile-like mouth opening, excessive elevation of the left upper lip, and occasional gum exposure, resulting in a mild “gummy smile (Figure 6) [4].” Due to the patient’s previous experience of facial rigidity after the initial injection, the injection dose was reduced to 50 U in the second treatment. Three weeks after the second treatment, the patient returned for a follow-up and was found to have incomplete correction of eyelid blinking, eye squeezing, and forced smile-like mouth opening during speech. An additional injection of 20 U was administered, and one week later, the symptoms resolved.

Figure 6: At the follow-up visit 7 months after the first injection, the state when speaking with eyes open.
| Injected sites | Muscle action | Injection level | Number of injection points | Injection dose per point (U) | Total dose (U) | |
|---|---|---|---|---|---|---|
| Frontal muscle | Brows raised, wrinkled forehead. | Intramuscular | 5 | 2 | 10 | |
| depressor supercilii, corrugat-or supercilii muscle | Pulling and gathering eyebrows inward and downward, resulting in longitudinal wrinkles between eyebrows. |
Subcutaneous | 6 | 2 | 12 | |
| Procerus | Synergistic nasal muscle contraction, the formation of nasal root transverse wrinkles | Subcutaneous | 2 | 2 | 4 | |
| Orbicularis oculi- muscle (inner and outer canthus) | Eyelid blink, twitching | Subcutaneous | 18 | Inside 1 Outside 2 |
36 | |
| Nasal muscle (transverse) | Shrugging nose, synergistic eyebrow muscle contraction | Subcutaneous | 2 | 2 | 4 | |
| Lifting upper lip nasal alar muscle (upper segment) |
Enlarge the nostrils, cooperate with nasal muscle contraction, and form oblique wrinkles on the back of the nose | Subcutaneous | 2 | 2 | 4 | |
| Orbicularis oris muscle (upper and lower lip) | Lip twitching, forming repeated pursing action. | Subcutaneous | 8 | 1 | 8 | |
| Mentalis | Participate in lip twitching and pursing action. | Subcutaneous | 2 | 1.5 | 3 | |
| Lifting upper lip nasal alar muscle (middle and lower segment) | The upper lip is pulled up,and the zygomatic muscle and the upper lip muscle are contracted to form a false smile and a gummy smile. | Subcutaneous | 2 | Lift 3 Right 2 |
5 | |
| levator muscle of upper lip | Participate in the formation of false smile, gummy smile. | Subcutaneous | 2 | 2 | 4 | |
| greater zygomatic muscle | Form false smile, gummy smile. | Subcutaneous | 2 | Lift 3 Right 2 |
5 | |
| Risorius | Stretch the mouth angle outwards. | Subcutaneous | 2 | Lift 2 Right 1 |
3 | |
| Depressor muscle of lower lip | Pull down the mouth angle, cooperate with other perioral | muscle contraction to form a false smile appearance. | Subcutaneous | 2 | 2 | 4 |
| Depressor anguli oris (left) | Muscle strength is stronger than the contralateral side, resulting in false smile when the mouth angle left. |
Subcutaneous | 1 | 2 | 2 |

Figure 7: Injection point position.
Dystonia is defined as a movement disorder characterized by sustained or intermittent muscle contractions that result in abnormal, repetitive movements or postures, or both. The clinical manifestations are diverse: it can present as simple blepharospasm and gradually develop into bilateral or oromandibular dystonia, even involving muscles such as the tongue, pharynx, and neck. When blepharospasm is combined with oromandibular dystonia, it is also referred to as MS [2]. Blepharospasm is caused by dystonic contractions of the orbicularis oculi, often accompanied by contractions of the procerus and corrugator muscles. The onset is usually insidious, beginning with eye irritation or dryness followed by excessive blinking, particularly in bright light [5]. Studies have shown a higher prevalence in countries with high sun exposure compared to regions with low sun exposure [6]. The common characteristics of this syndrome are well-known, but its manifestations are varied. Different eponyms such as “Breughel syndrome,” “Wood syndrome,” “Blepharospasm plus,” “Segmental cranial dystonia,” and “Segmental cranio-cervical dystonia” have been used to describe this entity with numerous anatomical variations [2]. MS can be divided into primary and secondary types based on distinct clinical manifestations and etiologies. The pathogenesis of MS may be associated with dysfunction of gamma-aminobutyric acid neurons, cholinergic hyperactivity, dopamine receptor hypersensitivity, or dopaminergic neurotransmitter imbalance [1]. To date, the exact etiology and pathogenesis of MS remain unclear, and there is no fundamental cure. Conventional treatment methods include oral medications such as antidopaminergic drugs, anticholinergic drugs, gamma-aminobutyric acid drugs, and antidepressants. However, due to the lack of strong evidence confirming the efficacy of oral medications, along with numerous side effects and poor long-term tolerance, these treatments have limitations [7]. Deep Brain Stimulation (DBS) is a novel treatment method for MS. It is a beneficial treatment option for patients who have unsatisfactory efficacy with oral and/or injection drugs, or who are intolerant to adverse drug reactions and have severe symptoms affecting daily life. DBS is characterized by being minimally invasive, reversible, controllable, and personalized [8]. However, the effectiveness and safety of surgery are influenced by many factors, and the high cost makes it unaffordable for many patients.
In this case, the patient exhibited high tension in the corrugator supercilii, procerus, orbicularis oculi, nasal, and orbicularis oris muscles in the closed-eye static state. In the open-eye dynamic state, high tension was observed in the frontalis, levator labii alaeque nasalis, levator labii superioris, levator anguli oris, zygomaticus major, zygomaticus minor, depressor labii inferioris, and depressor anguli oris muscles. It was found that the muscles showing high tension in both static and dynamic conditions were exactly antagonistic muscles. In treating the patient’s leftward deviation of the mouth corner, based on the principle of muscle balance between antagonistic muscles, BTXA was used to re-establish a new dynamic balance among these muscles. The injection doses of the muscles on both sides of the face were adjusted, achieving satisfactory results.
MS is a rare movement disorder that often leaves patients struggling with facial spasms and involuntary movements, severely impacting their quality of life. The application of BTX-A can effectively alleviate the excessive tension of facial muscles in patients and improve their psychological state. In the field of plastic surgery, the principle of wrinkle elimination and facial contour improvement through BTX-A injections, which blocks nerve signals to reduce local muscle activity, is also applicable to MS treatment. By precisely controlling the injection sites, it is possible to effectively alleviate patient symptoms and help them return to normal life. However, despite its generally favorable safety profile, BTX-A injections carry inherent risks, primarily due to the complex and variable anatomy of the facial region. These risks stem from the intricate structures and anatomical differences at the injection sites among individuals [12]. The function of facial expression muscles is more complex. The action of an expression usually requires the coordinated contraction of several muscles, such as the eyebrow complex, or an area with multiple muscles, such as lip movement. Among these muscles, there are both synergistic and antagonistic muscles. Comprehensive consideration is needed during injection to avoid muscle imbalance between antagonistic muscles, which can result in strange and stiff expressions [13]. Most facial expression muscles span multiple anatomical layers from their origin to insertion, with most inserting into the dermis. Due to the lack of fascial wrapping around the expression muscles, the dispersion of BTX-A injections increases. Selecting the appropriate dilution concentration and precise injection can reduce the dispersion range and produce the desired clinical effect.
In summary, the clinical use of BTX-A injections for MS treatment offers significant advantages in improving patients’ quality of life, reducing self-confidence damage, and alleviating social psychological disorders. The treatment is convenient, with safe and effective repeated treatments, rapid onset, long-lasting effects, and minimal economic burden on patients, making it a clinically promising method for this condition.
Conflict of interest: No other author has reported a potential conflict interest relevant to this article.
Funding: This research did not receive any specific funding from external sources, including government grants, industry sponsorships, or support from non-profit organizations. The authors carried out this work using their existing institutional resources and personal time and efforts, without any financial influence or support that could potentially create a conflict of interest.