Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Paulina Gisman
Clinical Ward of Paediatric Surgery and Urology, Regional Specialised Childrens Hospital in Olsztyn, Poland.
Email: gismanp@gmail.com
Received: Sep 24, 2025 Accepted: Nov 07, 2025 Published: Nov 14, 2025
Citation: Gisman P, Pulinski M, Janowicz T, Szostawicki M. Surgical repair of extensive myelomeningocele using integra® dermal regeneration template. Ann Case Rep Med Images. 2025; 2(2): 1048.
Copyright: Gisman P et al. © All rights are reserved
Myelomeningocele (MMC) is a severe congenital malformation of the central nervous system arising around the fourth week of fetal life due to neural tube closure failure. This defect results in an open communication between the neural placode and the external environment, causing neurological impairments and organ dysfunction. Despite advances in prenatal diagnostics, folic acid prophylaxis, and fetal surgery, children with this condition continue to be born.
Management of MMC requires urgent surgical intervention to close the defect and prevent infection. In extensive lesions, primary closure may be challenging due to insufficient surrounding tissue, making regenerative materials a valuable adjunct.
We report a female neonate with a large MMC extending from the interscapular to sacral regions. The neural placode was dissected, tubularized, and covered with dura, after which the wound was overlaid with a dermal regeneration template (Integra®). After four weeks, the matrix was covered with a skin graft, followed by an additional graft to cover areas of granulation tissue.
This approach, combining a dermal regeneration matrix with delayed skin grafting, offers an alternative strategy for managing extensive MMC defects, minimizing tension on surrounding tissues, and reducing the risk of wound complications.
Keywords: Myelomeningocele; Dermal regeneration template; Skin graft.
Myelomeningocele (MMC) represents the most prevalent congenital malformation of the central nervous system. It results in permanent disability, manifesting as paralysis of the lower extremities and impaired function of the anal and urinary sphincters. The severity of motor deficits correlates with the level of the spinal defect. The lesion most frequently involves the lumbar and sacral regions of the spine, while thoracic involvement is less common [5].
Currently, the incidence of births complicated by MMC has declined, due to availability in prenatal diagnostics and the advancements of fetal surgical interventions. Prenatal MMC detection is feasible via obstetric ultrasound as early as 12–13 weeks of gestation, and is readily identifiable during the second trimester.
Myelomeningocele develops through a two-stage process (the two-hit theory). The first stage involves disrupted neurulation of the spinal cord between the 4th and 8th week of gestation. The second stage consists of secondary injury to the exposed spinal cord, resulting from exposure to amniotic fluid and mechanical trauma against the uterine wall. Accordingly, it is believed that prenatal surgical repair can minimize the secondary stage of injury. Fetal surgery is typically performed between 21 and 26 weeks of gestation.
Despite advances in diagnostic techniques, children are still born with MMC without a prior diagnosis Several postnatal surgical techniques have been described, including primary skin closure, local skin flaps, musculocutaneous flaps, and skin grafts. Limberg latissimus dorsi musculocutaneous flap is a common type of repair for extensive defects. It is a transposition flap utilized following a standard dural repair. The technique involves converting the defect margin into a parallelogram, with incision and dissection carried out above the muscle fascia, allowing the flap to be transposed over the defect. Limberg flaps provide a reliable reconstructive option when primary closure is not feasible [7,8].
Dermal Regeneration Templates (DRT) have been successfully utilized in conjunction with flap procedures both prenatally and postnatally, demonstrating favorable outcomes [9]. The Integra Dermal Regeneration Template is a bilayer biomaterial composed of a collagen–chondroitin sulfate matrix with controlled pore size and degradation rate, which promotes cell migration, neovascularization, and restoration of the dermal structure [2,4,11].
We present a case of a female newborn with an extensive myelomeningocele extending from the interscapular region to the sacral area. The diagnosis was established by ultrasound performed just prior to delivery and confirmed by fetal MRI scan. The infant was also diagnosed with hydrocephalus, holoprosencephaly, patent foramen ovale, and patent ductus arteriosus. Following birth and thorough clinical examination, a treatment plan for surgical repair and reconstruction was established. Given the extensive surface area of the defect, coverage with two Limberg flaps was deemed necessary. However, this approach was associated with a high risk of wound disruption and leakage, as well as the potential for flap ischemia. Furthermore, the procedure would likely have resulted in considerable deformity.
Repair was performed using a dermal regeneration template. The neural plate was dissected, tubularized, and completely covered with dura mater, the wound was then covered with Integra Dermal Regeneration Template. Hydrocephalus was relieved, by placing Ventriculoperitoneal Shunt (VPS).
The wound was closed with Negative-Pressure Wound Therapy (NPWT). The pressure was set at a continuous pressure of 40 in order to help splinting of the DRT and to minimise loss of CSF. NPWT works by stimulating angiogenesis, continuous or intermittent suction removes bacteria and contaminants, creates a closed system, reducing external contamination. Additionally, we used a dressing with nanocrystalline silver (Acticoat Flex 3) as another barrier against bacteria. After a 4-week period that allowed the regeneration of the matrix, the patient returned to the operating theatre, the outer silicone layer had been removed. An 0,15 mm was harvested from the back area and it was not affixated. The graft was secured in place by Negative-Pressure Wound Therapy (NPWT).
Over the course of one month daily sterile dressing changes were carried out to facilitate complete healing of the graft. We encountered a challenge in maintaining wound hygiene. Due to extensive damage to the nervous system, the child presented with anal sphincter insufficiency, which resulted in uncontrolled fecal contamination of the wound. The healing process was complicated by granulation tissue in the areas not covered by the skin graft.
Four weeks after the initial skin graft, another surgical procedure was performed. An 0,2 mm thick skin graft had been placed on the areas covered in granulation tissue. At 2 months follow-up following the initial repair, the patient demonstrated continued good progress with a stable graft site.

Figure 1: A newborn 24 hours after birth presenting an extensive myelomeningocele extending from the interscapular region to the sacral area.
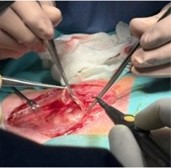
Figure 2: Operation within 48 hours of birth. Dissection and tubularization of the neural plate.

Figure 3: Post operation MMC is covered by dermal regeneration template.

Figure 4: Removal of the outer silicone layer 4 weeks post primary operation.

Figure 5: First skin graft.

Figure 6: The skin graft after 5 days.

Figure 7: Repair of skin graft over a period of a month.

Figure 8: The 2nd skin graft in the areas of granulose tissue.

Figure 9: 2 months after initial repair follow-up.
Despite the availability of in utero myelomeningocele repair, postnatal reconstruction remains a procedure that must be performed. In some cases, the congenital defect is only identified shortly after birth due to inadequate prenatal care. The primary objectives of myelomeningocele repair are the closure of neural elements and the achievement of stable soft-tissue coverage. Techniques for soft-tissue reconstruction vary according to the size of the defect, ranging from primary closure to musculocutaneous flap procedures. Closure of large defects often necessitates the use of such flaps; however, these approaches require donor sites that can be extensive. This approach leads to severe deformity. Larger flaps carry an increased risk of necrosis and impaired wound healing, which may compromise dural repair.
In a case study Hasham et al. [1] used two layers of a NovoSorb BTM which is also an artificial dermal template. The difference being Integra(®) DRT is animal-derived and more widely used than the NovoSorb™ Biodegradable Temporising Matrix, a fully synthetic alternative [10].
Similarly to our approach North WD et al. [3] used Integra DRT. North WD and Hasham both cover the templates with 8/1000 inches (0,2 mm) skin grafts after a healing period of 21-16 days. Likewise, after 27 days we performed the first skin graft, however we used a 0,15 thick skin graft. Both of these case studies describe using artificial dermal templates because of the extensity of the defect.
Dermal Regeneration Templates (DRTs) offer an alternative strategy for the closure of extensive defects. This approach has been shown to be safe, although it presents specific challenges, including the need to maintain the child in a prone or lateral position and the risk of infection due to the proximity of the anus.
Using dermal regeneration template can be used as an alternative treatment in myelomeningocele, especially in cases where the area of the defect is extensive and classic methods would require extensive operations.