Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Celeste Pugliaro
Respiratory and Allergy Clinic, IRCCS Policlinico San Martino, University of Genoa, Genoa, Italy.
Email: cpugliaro@gmail.com
Received: Sep 01, 2025 Accepted: Nov 04, 2025 Published: Nov 11, 2025
Citation: Pugliaro C, Milano V, Shyti G, Marco FD, Braido F. Pleural effusion as a clinical presentation of whipple disease: A case report. Ann Case Rep Med Images. 2025; 2(2): 1047.
Copyright: Pugliaro C et al. © All rights are reserved
Background: Whipple disease is a rare condition caused by the actinomycete Tropherima whipplei, ranging from asymptomatic carriage to chronic localized and systemic infections. The long and nonspecific prodromal symptoms often lead to misdiagnosis and delays in the administration of therapy, causing complications.
Case presentation: We present the case of a 64-year-old male with a history of type 2 diabetes, asbestos exposure, tobacco use, chronic arthritis, and unintentional weight loss of 10 kg over two years. He presented to the pneumology clinic with acute respiratory distress, right-sided pleuritic chest pain, and evidence of chronic bilateral pleural effusion. Imaging, including 18F-FDG PET/CT, revealed mild radiotracer uptake in the left lower lobe and pleural abnormalities indicative of inflammation.
Further investigation revealed systemic involvement, leading to the diagnosis of Whipple disease. This case showed multi-organ involvement: pleuro-pulmonary (pleural effusion and parenchymal thickening), cardiac (native valve endocarditis on aortic and tricuspid valves), gastrointestinal (malabsorption and weight loss), and neurological (PCRpositive cerebrospinal fluid for T. whipplei). Definitive diagnosis was confirmed by duodenal biopsies, with positive PCR results for T. whipplei in blood, cerebrospinal fluid, saliva, and pleural fluid.
Conclusion: This case illustrates an atypical presentation of Whipple disease with pleuro-pulmonary involvement. It underscores the diagnostic challenges posed by its variable symptoms and highlights the need for a multidisciplinary approach to ensure timely diagnosis and prevent disease progression.
Keywords: Pleural effusion; Bilateral pleural effusion; Whipple disease; Tropherima whipplei; Rare causes of pleural effusion.
Abbreviations: 18F-FDG PET: 18 Fluorodeoxyglucose Positron Emission Tomography.
Whipple disease is a rare infectious condition with an annual incidence of less than one case per million [1], primarily affecting middle-aged men [2]. The infection likely occurs via the orooral or fecal-oral route and is often asymptomatic [3]. It is caused by Tropheryma whipplei, ranging from asymptomatic carriage to symptomatic primary infections [1]. Key symptoms include weight loss, musculoskeletal discomfort, and gastrointestinal issues [4]. Chronic Whipple disease may also involve lung infiltration [5], cardiac symptoms, and central nervous system complications [2]. Nonspecific prodromal symptoms often lead to misdiagnosis and treatment delays [1-6].
A 64-year-old male with bilateral pleural effusion and dyspnea was referred for evaluation. The patient reported a 10 kg weight loss and loss of appetite over two years, a smoking history (former smoker, 6 packs/year), occupational asbestos exposure, type 2 diabetes, and rheumatoid arthritis diagnosed two years prior. One month prior to the outpatient visit, a thoracic CT scan (Figure 1) performed due to right thoracic pain revealed bilateral pleural effusion and two left pulmonary opacities.
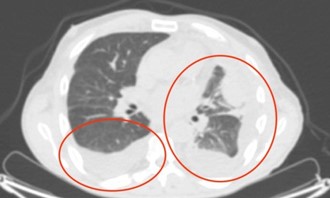
Figure 1: Thoracic CT scan prior to the first visit.
“Profuse pleural effusion in the left lung field, with intrascissural involvement; moderate pleural effusion in the right basal area. There are two areas of parenchymal thickening, both in the lower left lobe and in the lingula, characterized by uneven contrast enhancement with contiguous bronchiolitis, extending caudally to the ipsilateral pulmonary base, where they appear without cleavage. These findings are of unknown nature (productive lesion? inflammatory?) and warrant clinical-laboratory correlation, re-evaluation with a CT PET scan, and specialist evaluation. No focal parenchymal lesions are noted on the right.
Dystrophic bubbles in the lingula and ipsilateral upper lobe. Bilateral basal fibrotic striae. A nodule (approximately 6 mm) is noted in the middle lobe, which cannot be characterized due to its size and warrants follow-up. The trachea and large bronchi are patent. Hilarmediastinal lymphadenopathy of approximately 18 mm with a short axis of 11 mm and subcentimetric lymph nodes along the left internal mammary chain; concomitant axillary lymph nodes and caudally to the pectoral muscle, with a maximum diameter of approximately 10 mm bilaterally.”
A CT/FDG PET scan (Figure 2) performed two weeks before the visit showed slightly increased radioactive uptake (SUV max 2.6).
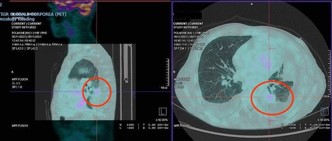
Figure 2: 18F-FDG PET scan two weeks before hospitalization.
“The PET/CT scan shows minimal accumulation of the tracer, at the limits of diagnostic significance, localized to the known pulmonary thickening in the lower left lobe (SUVmax 2.6). Findings cannot be further characterized on the basis of PET alone and warrant further targeted diagnostic investigation. Limited by the resolution capacity of the method (4 mm), no areas of radiopharmaceutical accumulation are evident in the body segments examined.
No accumulation of the tracer is seen in the known left lung parenchymal thickening in the lingular region. No accumulation of the tracer is observed in the massive bilateral apico-parietobasal pleural effusion, more evident on the left, which has increased compared to the previous CT scan. No significant accumulation is seen in the mediastinal lymph nodes or in the left internal mammary area.”
Conclusions: The exam is negative for disease with high glucose metabolism. The left lung finding, at the limits of diagnostic significance, cannot be further characterized on PET alone and warrants clinical judgment and targeted diagnostic investigation.
We decided to admit the patient to our respiratory diseases ward to continue investigations and start medical treatment. The abdominal-thoracic CT scan performed at hospitalization (Figure 3) identified pathologic lymph nodes along the left internal mammary chain and significant bilateral pleural effusion, primarily on the left. His arterial blood partial pressure of oxygen was 55 mmHg.
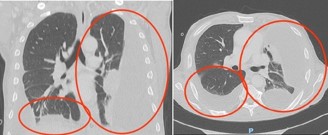
Figure 3: Thoracic-abdominal CT scan performed at the beginning of hospitalization.
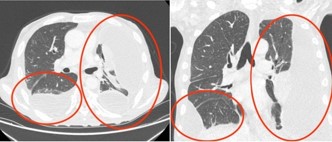
Figure 4: Abdominal-thoracic CT scan performed one month after hospitalization.
“No lymphadenopathy in the supraclavicular, axillary, or hilar-mediastinal regions. Small internal mammary lymph nodes on the right and slightly larger ones on the left, corresponding to the non-capturing findings on PET. Bilateral pleural effusion of moderate severity, with a maximum thickness of 47 mm on the right and 77 mm on the left; the pleura is slightly and uniformly thickened and hyperemic, with no solid nodules exhibiting typical features of a progressive lesion. The lung parenchyma shows extensive areas of atelectasis on the left and passive basal atelectasis on the right.
No alterations in the liver, spleen, pancreas, kidneys, or adrenal glands. No abdominal lymphadenopathy or expansive pelvic lesions. Subtotal thrombosis of the inferior vena cava in its most caudal section, partially extending to the common iliac veins. Distended bladder with regular walls. No peritoneal effusion.”
An exploratory thoracentesis drained 500 cc of hematic fluid, resulting in clinical improvement. In the cytological examination, no atypical elements were noted; the physicochemical analysis indicated an exudate, and cultures yielded negative results. A few days later, the patient exhibited worsening dyspnea, hypoxemia, and fever. A SARS-CoV-2 test was positive, while tests for respiratory viruses and bacteria were negative. He received Remdesivir for five days, resulting in clinical improvement. Another exploratory thoracentesis drained 1500 cc of hematic fluid, again providing benefit. A thoracic surgery consultation was requested due to chronic pleural effusion and asbestos exposure. The patient was scheduled for thoracoscopy to obtain pleural biopsies and possibly perform pleurectomy or chemical pleurodesis with talc. The patient repeated the abdominalthoracic CT scan after one month (Figure 4).
“Compared to the previous CT scan, the lymph nodes along the internal mammary chain on the left side are unchanged. No significant lymphadenopathy in the other mediastinal stations. The conspicuous bilateral pleural effusion, partly sacculated and greater on the left side, is essentially unchanged. Consensual lung atelectasis. Overall, the thoracic findings are essentially unchanged compared to the previous CT scan.
Presence of a caval filter. Slightly reduced thrombotic hypodensity in the IVC and common iliac veins. No obvious alterations in the liver, pancreas, spleen, adrenal glands, or kidneys (small bilateral renal cysts). No bilateral hydronephrosis.
Minimal periportal effusion. The current examination shows concentric edematous thickening of a reactive-inflammatory appearance in the ascending and proximal transverse colon.”
A cardiology evaluation revealed a hypertrophied left ventricle, an ejection fraction of 60%, and suggestive images of endocardial vegetations at the aortic and tricuspid valves. An infectious disease consultation recommended blood cultures, immunophenotyping, and serological tests. Blood results showed positivity for Tropheryma whipplei PCR, after which a duodenal biopsy was performed, confirming a diagnosis of chronic systemic Whipple disease with pleuro-pulmonary, cardiac, duodenal, and neurological involvement. The patient tested positive for T. whipplei in PCR analysis of blood, cerebrospinal fluid, saliva, and pleural fluid. He was initially treated with 2 g of intravenous ceftriaxone, followed by 960 mg of oral cotrimoxazole twice a day; after a few weeks, the treatment was changed to 200 mg of oral doxycycline per day in combination with 600 mg of oral hydroxychloroquine per day, for 1 year. The patient also underwent left pleural decortication and thoracotomy due to pleural empyema.
Whipple disease is a rare infectious condition with an annual incidence of less than one case per million people [1] and primarily affects middle-aged men [2]. It is a chronic infection caused by the actinomycete Tropheryma whipplei, ranging from asymptomatic carriage to symptomatic primary infections, chronic localized infections, and the systemic chronic infection known as classical Whipple’s disease [2]. The initial infection likely occurs through the oro-oral or fecal-oral pathway and is generally asymptomatic [3]. The most common symptoms are weight loss, musculoskeletal discomfort, and gastrointestinal symptoms such as diarrhea and abdominal pain. Arthralgia and arthritis typically present as the initial symptoms, occurring several years before gastrointestinal symptoms [4]. In this case report, the patient initially showed weight loss of 10 kg, loss of appetite, and arthritis over the past two years.
Patients with chronic Whipple disease rarely exhibit pulmonary involvement, such as pleural effusion, lymphadenopathy [6], and lung infiltration [5]. Few case reports describe pulmonary involvement mimicking sarcoid-like lung disease, initially responding to glucocorticosteroids [7]. In this patient, the pulmonary involvement included pleural effusion and left pulmonary opacities with slight uptake of radioactive material (SUV max 2.6) on 18-FDG PET; pleural biopsies showed histopathological features consistent with pleural empyema. Other rare symptoms include cardiac involvement (negative blood-culture endocarditis) [2]. In this case report, the patient had endocardial vegetations localized to the aortic and tricuspid valves, with mild associated valve regurgitation and an ejection fraction of 60%. Central nervous system (CNS) involvement is also described in Whipple disease and is the most severe complication. Although they are difficult to identify as characteristic of classic Whipple’s disease, nonspecific headache and cognitive failure are potential signs of CNS involvement. Specific CNS symptoms, such as oculofacioskeletal myorhythmia or progressive supranuclear ophthalmoplegia with oculomasticatory myorhythmia, are considered pathognomonic for Whipple’s disease [4]. In this case report, the patient underwent a lumbar puncture with a positive PCR result for T. whipplei in the cerebrospinal fluid, despite being asymptomatic.
In systemic Whipple disease, the long and nonspecific prodromal symptoms often lead to misdiagnosis and delays in the administration of therapy, causing complications. Histopathology of duodenal samples is the gold standard for diagnosing Whipple disease: two tissue samples must be positive, and for Whipple’s disease to be excluded, two biopsy results must be negative [4].
Whipple disease treatment includes initial therapy with 2 g intravenously once a day of ceftriaxone; alternatively, 1 g intravenously three times a day of meropenem. Long-term therapy consists of 960 mg orally twice a day of cotrimoxazole; alternatively, 200 mg orally per day of doxycycline in combination with 600 mg orally per day of hydroxychloroquine, for one year [4]. In summary, in this case report, the patient was found to have chronic systemic Tropheryma whipplei infection, Whipple disease, with multiple localizations: pleuro-pulmonary (pleural effusion and pulmonary thickening), cardiac (native bivalvular aortic and tricuspid endocarditis), duodenal (weight loss and malabsorption), and neurological (positive PCR test for T. whipplei in the cerebrospinal fluid). Finally, the patient underwent left pleural decortication and toilette of the pleural cavity for pleural empyema, a complication of pleural involvement. This case highlights the importance of differential diagnosis in patients with pleural effusion. Atypical systemic involvement necessitates consideration of rare systemic diseases for timely diagnosis and treatment, potentially preventing invasive interventions like decortication.
This case underlines the importance of considering Whipple disease in the differential diagnosis of unexplained pleural effusion, particularly when associated with systemic signs such as weight loss, arthritis, and cardiac involvement. While pulmonary manifestations are rare in Whipple disease, this case report highlights that pleuro-pulmonary involvement can occur and lead to significant complications requiring surgical intervention. To prevent permanent consequences, early detection through histological testing and prompt initiation of appropriate antibiotic therapy are crucial. Ultimately, this case illustrates the need for a multidisciplinary approach in patients with multisystem involvement and unclear etiology, in order to achieve timely diagnosis and prevent disease progression.