Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Tooke Lloyd
Department of Paediatrics and Child Health, University of Cape Town, Cape Town, South Africa.
Email: lloyd.tooke@uct.ac.za
Received: Sep 23, 2025 Accepted: Oct 28, 2025 Published: Nov 04, 2025
Citation: Philip AS, Tooke L. Perinatal tuberculosis – A rare but serious neonatal infection. Ann Case Rep Med Images. 2025; 2(2): 1046.
Copyright: Tooke L et al. © All rights are reserved
Perinatal Tuberculosis (TB) is a rare yet severe infectious disease which may affect neonates. This is a case of an infant who had non-specific manifestations of this disease, which mimic neonatal sepsis.
The focus of this case report is to increase the awareness of perinatal TB by describing a clinical case in a tertiary neonatology institution in South Africa, and providing information about which infants should raise suspicion about this rare condition. The clinical presentation, imaging, diagnosis and management of this condition is further discussed.
Keywords: Perinatal tuberculosis; Neonatal sepsis; Neonatology; Infectious diseases.
Abbreviations: CPAP: Continuous Positive Pressure Ventilation; CRP: C-Reactive Protein; CXR: Chest X-ray; MTB: Mycobacterium tuberculosis; NICU: Neonatal Intensive Care Unit; TB: Tuberculosis.
Perinatal Tuberculosis (TB) is a rare infectious disease which results in high morbidity and mortality. Infants younger than 3 months can be infected with TB congenitally or postnatally [1]. Congenital TB refers to the transmission of Mycobacterium Tu- berculosis (MTB) haematogenously via the umbilical vein or by foetal ingestion of infected amniotic fluid during birth [2]. It is relatively rare because it occurs in the setting of maternal TB endometritis or disseminated TB. Postnatally acquired TB oc- curs by the inhalation of MTB bacilli transmitted by aerosolized respiratory secretions from the infant’s mother or another pa- tient with cavitatory TB disease early after birth [3]. It is chal- lenging to distinguish between the two, so the term perinatal TB is used (i.e infants infected congenitally or within the first few days of life, and presenting within the first 3 months of life) [1].
A male infant, weighing 1145 g, was born at 28 weeks gesta- tion to a well 24-year-old, HIV negative, primigravida in a tertiary hospital in Cape Town South Africa. The mother presented with spontaneous preterm labour and due to a cardiotocographic trace depicting fetal tachycardia, the infant was delivered by cesarean section with Apgar scores of 7 and 9. The infant had respiratory distress at birth and was screened for sepsis, started on antibiotics (ampicillin, gentamycin) and admitted to the Neo- natal Intensive Care Unit (NICU) for Continuous Positive Pres- sure Ventilation (CPAP). By day 4 he had weaned to room air, did not require surfactant and was off antibiotics. The C-Reactive Protein (CRP) reading was 1 mg/L.
On day 16 of life the infant developed episodes of persistent tachycardia and respiratory distress, which raised concerns for possible late onset sepsis. The septic workup was again nega- tive (negative blood culture and CRP of 10 mg/L), and the infant completed 48 hours of second line antibiotics (meropenem) and was successfully weaned to room air after having been started on high flow nasal cannula.
However, on day 34, at a corrected gestational age of 33 weeks the infant had an episode of apnoea and returned to the NICU for CPAP and was again treated with meropenem. The blood culture was negative although the CRP was elevated (96 mg/L). A lumber puncture excluded meningitis. After an initial improvement, there was a further deterioration 12 days later when he became critically unwell. The infant now demonstrated hepatosplenomegaly and a further increased CRP (118 mg/L). Abdominal ultrasound revealed ascites with an enlarged liver and spleen with no focal lesions and no abdominal lymphade- nopathy. A lumber puncture excluded meningitis yet again with negative blood and cerebrospinal fluid cultures. Ascitic tap re- vealed a straw-coloured transudate. Chest X-ray (CXR)- see im- age) showed extensive infiltrates and parenchymal breakdown. Sputum was sent for GeneXpert testing, and he was started on 4-drug TB treatment.
Despite maximal ventilatory support which included high frequency oscillation, the infant developed persistent respira- tory failure and passed away 48 hours later. The sputum subse- quently detected isoniazid sensitive TB.
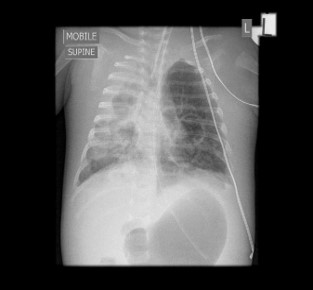
Figure 1: Infant’s CXR depicting extensive infiltrates and parenchymal breakdown.
The mother, who remained well and was not coughing re- ceived her own CXR which showed a miliary pattern (Figure 2).
Perinatal TB (congenital or postnatally acquired) is rare even in endemic areas, with non-specific clinical manifestations often leading to misdiagnosis or underdiagnosis [1].
During this infant’s neonatal course, he had multiple con- cerns of neonatal sepsis at day 16, 34 and 46 of life. However, his septic workup was non-specific, and cultures negative on all 3 occasions. This case report demonstrates how perinatal TB mimics neonatal sepsis and thus emphasizes the importance of considering perinatal tuberculosis as a differential diagnosis in neonates with recurrent concerns of neonatal sepsis not re- sponding to broad spectrum antibiotics.
Hepatosplenomegaly and respiratory distress are the most common manifestations of congenital tuberculosis followed by poor feeding, fever, failure to thrive, irritability, lethargy, cough, abdominal distension and low birth weight. Neonatal TB may present in the form of septicaemia, persistent or recurrent pneumonia, meningitis, lymphadenopathy, jaundice, ascites, disseminated intravascular coagulation, otitis media, osteo- myelitis, paravertebral abscess and cold abscess [2]. The initial presentation is often very similar to sepsis, so an unwell infant with a pneumonia or sepsis, raised CRP and negative serological tests, which fails to improve with broad spectrum antibiotics, should raise suspicion for perinatal TB [4]. Acquisition of tuber- culosis early in life increases the risk of extra-pulmonary spread [5]. Hepatosplenomegaly, conjugated jaundice, abdominal lymphadenopathy and a high lymphocyte count in cerebrospi- nal fluid are additional findings which support this diagnosis. A definitive diagnosis of TB is established by culturing MTB from a bodily secretion, fluid or tissue. Most neonates have miliary dis- ease pattern on CXR, adenopathy or parenchymal infiltrates [2].

Figure 2: Mother’s CXR depicting miliary TB.
As demonstrated in this case report, the assessment of ma- ternal risk factor for TB is vital in suspected perinatal TB as the diagnosis of congenital TB sometimes helps in the detection of undiagnosed maternal TB. Placental examination and culture for MTB should be done in symptomatic mothers [2]. HIV test- ing is also very important in suspected perinatal TB as these are often co-infections. Although our centre has a high maternal HIV infection rate, [6] perinatal TB remain rare. It is imperative to screen unwell mothers early as timely diagnosis and treat- ment are crucial to improve the prognosis of perinatal TB. How- ever, mothers may be deceptively well especially if they do not have cavitating pulmonary disease such as in this case.
Once cultures are obtained in a suspected perinatal TB, an- tituberculosis treatment should be started promptly before bacterial confirmation is received, as TB can progress rapidly in neonates. According to the World Health Organisation guide- lines for perinatal TB, the infant should be commenced on a 6-month treatment regimen (2 months Isoniazid (INH), Rifam- picin (RIF), Pyrazinamide (PZA), and Ethambutol (EMB), fol- lowed by 4 months of INH and RIF therapy 6. The treatment is tailored based on drug resistance testing. Prednisone (2 mg/kg/ day) should be administered for 4–6 weeks if TB meningitis is suspected [5].
The prognosis for perinatal tuberculosis is guarded, as the mortality rate of congenital tuberculosis even with effective treatment is 25-50%. Reasons for high morbidity and mortality associated with perinatal TB include the delayed diagnosis due to non-specific signs and symptoms, and the immature immune system of neonates making them high risk to develop active/ disseminated disease [4].
In conclusion perinatal tuberculosis is a rare but serious neonatal infection which is underdiagnosed, leading to severe morbidity and mortality. Due to its non-specific presentation, it should be considered in infants with concerns of neonatal sep- sis not responding to broad spectrum antibiotics, especially in endemic areas.
Informed consent: Written informed consent was obtained from the patient’s guardian prior to writing and publication of this case report. Ethical approval was obtained from the Univer- sity of Cape Town human research ethics committee.
Disclosure: The authors declare that they have no conflicts of interest concerning this article.