Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Hiroki Ohkoshi
Department of Respiratory Medicine, Yamanashi Kosei Hospital, 860 Ochiai, Yamanashi, yamanashi, 405-0033, Japan.
Email: hk.ohkoshi@gmail.com
Received: Oct 06, 2025 Accepted: Oct 25, 2025 Published: Oct 31, 2025
Citation: Matsuda K, Ohkoshi H, Homma K, Furuya S, Shimamura S, et al. A case of pulmonary nocardiosis complicated by pneumothorax during the treatment for interstitial pneumonia associated with rheumatoid arthritis. Ann Case Rep Med Images. 2025; 2(2): 1043.
Copyright: Ohkoshi H et al. © All rights are reserved
A 76-year-old man had been treated with prednisolone, tacrolimus, azulfidine, and nintedanib for interstitial pneumonia associated with rheumatoid arthritis for two years. A CT scan displayed a gradually enlarging cyst with wall thickening beneath the pleura in the superior segment of the left lung. In October 2023, he was admitted to our hospital due to a left pneumothorax. CT revealed that the rupture of a cyst was the cause of the pneumothorax. As he was unresponsive to treatment with thoracic drainage, pulmonary fistula closure surgery was performed using a muscle flap transplantation. Surprisingly, Nocardia species were detected in the pus within the cyst, leading to a diagnosis of pneumothorax caused by cyst rupture due to pulmonary nocardiosis. Although the patient had to discontinue Trimethoprim-sulfamethoxazole due to a drug eruption, we could successfully treat him with erythromycin based on the susceptibility test results. This case taught us several important lessons. First, we should consider nocardiosis as a differential diagnosis when evaluating nodules with cavities in immunocompromised patients. Second, species identification is crucial, as different Nocardia species exhibit varying antimicrobial susceptibility.
Keywords: Pulmonary nocardiosis; Pneumothorax; Nocardia veterana; Erythromycin.

Graphical abstract text: We report a rare case of pulmonary nocardiosis due to Nocardia veterana in an immunocompromised patient, which was complicated by a pneumothorax suspected to be the result of a ruptured cyst. After pulmonary fistula closure surgery, we observed an improvement in the thickening of the cyst’s wall 10 weeks after starting erythromycin monotherapy, indicating that the treatment was effective.
Nocardiosis is an opportunistic infection that primarily affects immunocompromised patients. It often involves the lungs, with patients presenting various imaging findings and clinical features [1]. Trimethoprim-Sulfamethoxazole (TMP-SMX) has been the first-line treatment for nocardiosis. However, its use is limited in some cases due to allergic reactions or drug resistance. There is insufficient evidence regarding second-line treatments when TMP-SMX cannot be used, and differences in antimicrobial susceptibility among Nocardia species have been reported [2].
In addition to the lack of adequate treatment options, there is limited knowledge regarding diagnostic clues from imaging findings and effective treatments for different Nocardia species.
In this report, we describe a case of pneumonia caused by Nocardia veterana complicated by pneumothorax. This case may represent the first reported instance of pulmonary nocardiosis successfully treated with erythromycin.
A 76-year-old male was brought to the emergency room in October 2023 with sudden-onset dyspnea and left shoulder pain. He had a history of interstitial pneumonia associated with rheumatoid arthritis and was on 5mg of prednisolone, tacrolimus, azulfidine, and nintedanib along with rabeprazole, atovaquone, and alendronate. The patient had no other significant medical history, but he had a smoking history of 20 cigarettes per day from ages 20 to 35. On examination, his oxygen saturation was initially in the 80% range at home but improved to 99% after initiating oxygen therapy with 3 liters per minute via nasal cannula. Chest auscultation revealed markedly decreased respiratory sounds on the left side. Laboratory tests showed a slight increase in the inflammatory response, with a white blood cell count of 9,350 /μL and a C-Reactive Protein (CRP) level of 1.23 mg/dL. Lactate Dehydrogenase (LDH) and sialylated carbohydrate antigen KL-6 levels were 254 U/L and 756 U/mL, respectively (Table 1), with no significant changes compared to his previous outpatient follow-up. Additionally, the Aspergillus antigen test was positive in June 2023. On the day of onset, a chest X-ray revealed the presence of a left pneumothorax (Figure 1). The initial CT scan upon admission demonstrated a cyst with wall thickening just beneath the pleura in the superior segment of the left lung (Figure 2A). A follow-up CT scan after insertion of a chest drain tube suggested that the pneumothorax was due to the cyst’s rupture. (Figure 2B). Prior CT scans from February 2021 to February 2023 indicated the cyst had gradually increased in size, with progressive wall thickening (Figure 2C, 2D).
Despite the chest drainage, the left lung did not fully expand, and the air leak persisted. We proceeded with surgery using a muscle flap to close the air leak. Based on the previous positive Aspergillus antigen test, we anticipated an Aspergillus infection; however, contrary to our expectations, Nocardia species were detected in the pus from the cyst. Further testing for Aspergillus, Mycobacterium avium complex, and other infections was negative.
We initiated the treatment of nocardiosis with TMP-SMX. Species identification later confirmed the presence of Nocardia veterana, which was susceptible to imipenem/cilastatin, amikacin, erythromycin, TMP-SMX, and linezolid (Table 2). Three weeks after the initiation of TMP-SMX, he developed skin rashes, which were suspected to be a drug eruption caused by TMP-SMX. As a result, we discontinued TMP-SMX and switched to oral erythromycin, since the species was susceptible to it and the patient’s general condition remained stable. After starting treatment with erythromycin, follow-up CT scans showed improvement in the thickening of the cyst wall, indicating a successful response to the oral erythromycin (Figure 2E, 2F).
| Laboratory tests | ||
|---|---|---|
| WBC | 9,350 | /Μl |
| Hb | 13.6 | g/dL |
| Plt | 16.6×104 | /μL |
| Neut | 63.5 | % |
| Mono | 4.5 | % |
| Lymph | 30.4 | % |
| Eosino | 1.2 | % |
| Baso | 0.4 | % |
| TP | 7.4 | g/dL |
| Alb | 3.7 | g/dL |
| LDH | 254 | U/L |
| BUN | 19.8 | mg/dL |
| Cre | 1.01 | mg/dL |
| eGFR | 55 | mL/min |
| CK | 321 | U/L |
| KL-6 | 756 | U/mL |
| PT time | 93.6 | % |
| PT-INR | 1.03 | |
| APTT | 28.1 | second |
| Fibrinogen | 340 | mg/mL |
| D-dimer | ≤0.5 | μg/mL |
| CRP | 1.23 | mg/dL |
| CK-MB | 1.5 | ng/dL |
| Troponin-I | <10 | pg/dL |
| NT-proBNP | 153.6 | pg/dL |
| β-D Glucan | 18.8 | pg/mL |

Figure 1: Chest X-ray on admission.
Chest X-ray on admission showed a left pneumothorax.
| Drugs | MIC(μg/ml) | Susceptibility |
|---|---|---|
| Penicillin G | >2 | Resistant |
| Cefotaxime | 16 | Intermediate |
| Ceftriaxone | 16 | Intermediate |
| Cefepime | 16 | Intermediate |
| Imipenem/cilastatin | ≤0.25 | Susceptible |
| Amikacin | ≤4 | Susceptible |
| Erythromycin | ≤0.25 | Susceptible |
| Clindamycin | 2 | Intermediate |
| Minocycline | 2 | Intermediate |
| TMP-SMX | ≤10 | Susceptible |
| Ciprofloxacin | >2 | Resistant |
| Linezolid | ≤2 | Susceptible |
Abbreviations: MIC: Minimum Inhibitory Concentration.
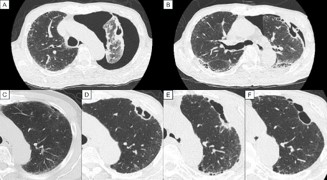
Figure 2: Chest computed tomography images. (A) On the day of admission, wall thickening of the cyst was observed along with pneumothorax. (B) A follow-up image after chest drainage revealed the rupture of the cyst. (C,D) The cyst beneath the pleura in the superior segment of the left lung gradually increased in size along with wall thickening. The images represent scans taken 20 months (C) and 8 months (D) before admission. The wall thickening of the cyst showed improvements 10 weeks after starting erythromycin. The images represent scans taken before erythromycin treatment (E) and 10 weeks after starting the treatment (F).
The patient’s condition remained stable for a year, allowing us to suspend the erythromycin treatment in October 2024. However, a CT scan in December 2024 exhibited a recurrence of wall thickening of the cyst and elevated CRP levels to 6.77 mg/dL. After resuming erythromycin treatment, the patient’s inflammatory response decreased within a month. We will continue erythromycin based on his laboratory results, imaging findings, and clinical manifestations.
In this case, we present a case of pulmonary infection caused by Nocardia veterana complicated by pneumothorax. This may also present the first instance of pulmonary nocardiosis successfully treated with erythromycin.
Nocardiosis commonly affects immunologically compromised patients, including those on long-term steroid or immunosuppressive therapy, HIV-positive individuals, cancer patients undergoing chemotherapy, and transplant recipients [3]. Differentiating nocardiosis from other infections is challenging because its clinical manifestations or radiographic features often resemble those of conditions like tuberculosis or various fungal infections [1]. Furthermore, some cases may involve mixed infections with these pathogens [4]. In general, radiographic features of nocardiosis can include nodules, consolidations, and cavities [5], with their frequency varying across different studies. Notably, pneumothorax associated with pulmonary nocardiosis is rare, with only a few cases reported [6]. Some studies have indicated that cavitations are more common in the immunocompromised group [7,8]. In our case, immunosuppressive therapy involving prednisolone, tacrolimus, and azulfidine was the significant risk factor for the cavities observed on chest CT scans. A previous report indicates that the use of steroids can lead to the expansion of pulmonary cavities in pulmonary aspergillosis [9]. In addition, there is a documented case in which a patient with pulmonary cavities developed a pneumothorax as a result of steroid treatment [10]. While reports of pneumothorax in patients with nocardiosis are limited, our case also suggests that steroids may contribute to the expansion of pulmonary cavities, potentially leading to pneumothorax. Therefore, it is crucial to consider nocardiosis when identifying pulmonary cavities in immunocompromised patients, while acknowledging the diverse radiological features associated with nocardiosis.
Successful treatment of nocardiosis requires accurate species identification and species-specific therapy. TMP-SMX is the first-line treatment for nocardiosis. However, alternative treatments guided by susceptibility tests are essential for patients with allergies to TMP-SMX. Zhao et al. revealed 10 antimicrobial susceptibility patterns, demonstrating the variety of drug susceptibility among each species [2]. In our case, mass spectrometry identified Nocardia veterana within a few weeks, allowing us to shift from TMP-SMX to erythromycin based on susceptibility test results after the onset of skin rashes caused by TMPSMX. Conventionally, 16 S ribosomal RNA gene sequencing is considered the gold standard for identification, though it is not always accessible. Recently, Matrix-assisted laser desorption/ ionization time-of-flight mass spectrometry has become an increasingly valuable, rapid, and reliable substitute [11]. While the characteristics of Nocardia veterana are mostly undescribed due to its rarity, we successfully selected the optimal treatment based on susceptibility test results. This adjustment led to noticeable improvements in the cyst wall and his stable clinical symptoms.
To our knowledge, there have been no previous reports demonstrating the successful treatment of nocardiosis with erythromycin monotherapy. Therefore, our case is particularly noteworthy as the first documented instance of successful treatment of Nocardia infection using erythromycin alone. This case highlights the importance of accurate species identification and susceptibility assessment for effective nocardiosis management.
In conclusion, it is essential to consider the possibility of nocardiosis when nodules with cavities are observed in the image of immunocompromised hosts. Furthermore, species identification and antimicrobial susceptibility tests are indispensable for effective treatment.
Ethics statement: Ethical review and approval were waived for this study due to it being a case report.
Consent: Informed consent was obtained from the patient.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Conflict of interest: None.
Disclosure statement: The authors declare no conflicts of interest.