Article Type: Case SeriesVolume 2 Issue 2
*Corresponding author: Basimbe Francis
Department of Surgery, Gastrointestinal Surgery Unit, St Francis Hospital Nsambya; Mother Kevin Post Graduate Medical School, Uganda Martyrs University Nkozi, Sona Laparoscopic Medical Centre Kampala, Uganda.
Email: basimbef@yahoo.co.uk
Received: Aug 25, 2025 Accepted: Sep 22, 2025 Published: Sep 29, 2025
Citation: Francis B, Allan M, Francis K, Iman HD, Cresent T, et al. Gastric antral perforation with a fish bone, laparoscopic surgical intervention in a sub-saharan setting: A case series. Ann Case Rep Med Images. 2025; 2(2): 1041.
Copyright: Francis B et al. © All rights are reserved
Foreign body ingestion is a common occurrence in clinical practice experienced in many parts of the world, especially among the pediatric population. However, their occurrence in an adult population is rare. Most foreign bodies in adults pass through the gastrointestinal tract without complications. Less than 1% cause perforation of the gastrointestinal tract and results in many complications including peritonitis, abscesses.
Some foreign bodies have been known to result in perforations of different parts of the gastrointestinal tract. Yet many of these foreign bodies have been seen to pass throughout the gastrointestinal tract without causing obstruction or perforation. We highlight two cases of gastric antral perforations with abscess complications seen and managed in our setting with laparoscopic surgery approach with excellent outcomes in both these cases, we did Initially a diagnostic laparoscopy, this revealed a walled off abscess, an antral perforation and a sharp fish bone foreign bodies that were identified and retrieved from the anterior antral perforations. Lavage and antral perforation repair with omentopexy were done for both these patients.
Conclusion: These are unusual cases of gastric antrum fishbone perforations with abscess formation seen in our setting and form the first set of documented cases managed laparoscopically with drainage of the abscess’s antral perforation repair and omentopexy with excellent outcomes.
Keywords: Gastrointestinal fishbone; Antral perforation; Laparoscopy.
Foreign body ingestion is a common occurrence in clinical practice experienced in many parts of the world especially among the pediatric population [8]. However, their occurrence in an adult population is rare. Most foreign bodies in adults pass throughout the gastrointestinal tract without event. Less than 1% cause perforation of the gastrointestinal tract and result in many complications including peritonitis, abscesses [7-10].
Some foreign bodies have been known to result in perforations of different parts of the gastrointestinal tract. Yet many of these foreign bodies have been seen to pass throughout the gastrointestinal tract without causing obstruction or perforation [7].
Cases of sharp foreign bodies causing injury in the upper gastrointestinal tract have been reported and these have been known to occur the pharynx, larynx and oesophagus. Gastric perforations from ingested foreign bodies in adults have not been commonly reported [7,9].
We highlight two cases of gastric antral perforations with abscess complications seen and managed in our setting with laparoscopic surgery approach with excellent outcomes.
We present a 49-Year-old male presented with longstanding abdominal pain that had worsened in 3 weeks mainly in the epigastric region, burning in nature and radiating to the back with associated loss of appetite.
There was no history of nausea or vomiting and no history of change in bowel habits and no history of abdominal distension.
An Upper GIT Endoscopy showed severe hyperemia and oedema of the antrum with Grade A GERD and a Hill I Hiatus Hernia.
On examination patient was afebrile, not pale, not jaundiced. Vitals: Blood pressure 142/92 mmHg, Pulse Rate 87 beats per minute, Temperature 37.2℃, SPO2 97% on room air & Respiratory Rate 19 breaths per minute.
Abdominal examination revealed normal fullness with marked Epigastric tenderness with guarding.
1. Laboratory investigatio CBC: WBC 5.5, # Neut 8.0 (2.0-7.5), # Lymph 1.4 (1.5-4.0), RBC 5.5, HB 14.7 g/dl, MCV 81.2 (76-96), MCH 26.6 (27-32) & PLT 300s done included
2. CRP 196.96 (0-50) mg/l.
A Contrast Abdominal CT scan revealed a foreign body with a fluid collection at the antrum walled off by the left lobe of the liver (Figures 1 & 2).
Contrast abdominal CT scans
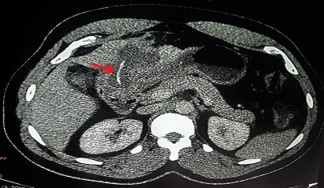
Figure 1: Shows a foreign body walled off by omentum (arrow) and the left lobe of the liver.
Following the investigations A decision was taken to do a diagnostic laparoscopy
At laparoscopy we found omentum sealed off at the antrum and pylorus and 1st part of duodenum and left part of the liver. Rest of the abdomen was normal.
Bluntly dissected, identified pus pockets and we drained 200 ml of pus.
We noted a fish bone about 4 cm in length with an antral perforation.

Figure 2: Shows foreign body walled off by the liver with surrounding abscess (arrow).
Drained, lavaged with 2 litres of normal saline and did omentopexy with vicryl 2/0 to close the antral perforation.
Patient was admitted to a High Dependence Unit (HDU) and managed with analgesia, antibiotics and had an excellent recovery and was discharged after 2 days.
A.M a 58-Year-old presents with severe Abdominal pain for 2 weeks, He is a Known Hypertensive for 3 years ambulating on clonidine, telmisartan, eplerenone, Rosuvastatin, clopidogrel, had a stroke 3 years ago and fully recovered. He Presented with a 2-week history of abdominal pain, moderate to severe. Non radiating involving right flank and epigastric, worse on eating relieved by fasting.
Reports nausea and vomiting on feeding, also reports loose motions for the same period however, no difficulty swallowing, no constipation.
Clinical examination
Vitals: Blood Pressure 156/71 mmHg, Pulse Rate 95 beats per minute, SPO2 97% on room air, Respiratory Rate 16 breaths per minute, Temperature 37.8℃ and Random Blood Sugar of 9.1 mmol/L
Abdominal examination found Normal fullness of the abdomen with generalized tenderness with no guarding & normal bowel sounds in pitch and frequency.
Laboratory investigations blood grouping: A Rh D positive, HIV – Seronegative, CBC: WBC 16.42, # Neutrophils 13.68 (2.07.0), # Lymphocytes 0.85 (1.5-4.0), RBC’s 4.4, Hb 13.8 g/dl, MCV 88.6 & MCH 31.4.
Liver function test’s: ALP 242 (40-130), ALT 49.2 (0-40), AST 38.3 (0-51), GGT 341 (8-61), Albumin 35.6, Total Bilirubin 17.4 (0-15.39), Direct Bilirubin 9.8 (0.34.2), & Total protein 72.5.
Renal functional tests: Cr 66 (62-106), Na+ 131 (136145), K+ 4.32 (3.5-5.1), Cl93.1 & Urea 2.2 (2.14-8.21),
A contrast abdominal CT scan found a foreign body at the antrum walled off by the left Lobe of the liver with an associated abscess walled off (Figures 3 & 4).
Contrast abdominal CT scans

Figure 3: Abdominal CT scan shows a foreign body partly embedded in the liver (arrow).
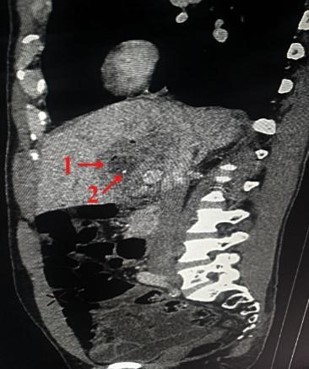
Figure 4: Foreign body perforated through antrum into the left lobe of the liver (arrow 1) with an associated abscess (arrow 2).
A decision was taken to do a diagnostic laparoscopy.
Found an omentum matted at the pylorus and 1st part of duodenum and left part of the liver. Rest of the abdomen was normal.
Bluntly dissected, identified pus pockets drained 100 ml of pus.
Also noted a fish bone about 10cm in length with an anterior antral perforation (Figure 5).
Drained and lavaged with two liters of normal saline and placed an omental patch at the site of the antral perforation and secured it with vicryl 2/0.
The patient made an excellent recovery and was discharged in 4 days.

Figure 5: Shows a diagnostic laparoscopic image of a fish bone (arrow 1) at the right liver lobe (arrow 2).
The stomach plays a critical role in the digestive process of ingested food, it is influenced by both hormonal and neurological signals that regulate motility and appetite as well.
While anatomically it is composed of different parts. Physiological functionality divides it into the upper portion which mainly works as a reservoir and the lower portion whose main function is churning to mix food with digestive juices and eventual propulsion of contents into the duodenum [2].
This lower portion is subject to many signals that are initiated from the gastric pacemaker, and these are aimed at digestion and propelling the contents out of the stomach [2].
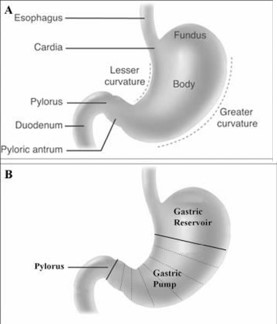
Figure 6: The anatomical regions (A) and functional regions (B) of the stomach. (Adapted from: Mercer DW, Liu TH, Castaneda A. Anatomy and Physiology of the stomach. in Zuidema GD, Yeo CJ: Shackelford’s Surgery of the Alimentary Tract. 5th ed, Vol II. Philadelphia: Saunders 2002, p 3. Copyright Elsevier).
Gastric motility in the lower portion is regulated by a strong slow wave, a 3 cycle per minute depolarization of the smooth muscle regulated by the Interstitial Cells of Cajal (ICC) specialized located along the mid portion of the greater curvature [2]. Once this is initiated it is much stronger and faster than the lesser curvature waves that are meant to terminate at the pylorus [3]. Both cases seen in our setting had perforations at the antral lesser curvature.
It can therefore be hypothesized that the foreign body to sharply impel and subsequent perforation at the lesser curvature by the sharp foreign body is because of these antral waves initiated by the ICC at the mid portion of the greater curvature.
From the cases none of the patients had a recollection on when they had ingested the fish bone and therefore it was not possible to establish exact timelines involved. However associated abscesses are an indication that this may have been over weeks to months.
As noted, Gastric motility is as a result complex mechanisms that have both hormonal and neurological coordination.
None of our patients were known to have disorders of gastric motility prior to the presentation in hospital and this can be further emphasized by the lack of criteria for diagnosing motility disorders based on the Rome III Criteria of Functional Dyspepsia [4].
Management
In both these cases, we did a diagnostic laparoscopy after investigations. This revealed a walled off abscess, an antral perforation and a sharp fish bone foreign body that was identified and retrieved from the anterior antral perforation.
Lavage was done of the cavity and antral perforation repair with omentopexy.
These are unusual cases of gastric antrum fishbone perforations with abscess formation seen in our setting and form the first set of documented cases managed laparoscopically with drainage of the abcesses antral perforation repair and omentopexy with excellent outcomes.
Consent: All authors of this article consented to have this work published.
Consent to participate: The patients presented in this article gave consent to participate in this article and to have their images and results as part of the publication.
Funding: We declare that there has not been any significant financial support received that can influence the outcome.
Data availability statement: All information regarding these cases and imaging photos are available at St Francis Hospital Nsambya Department of Surgery.
Conflict of interest: We declare no conflict of interest.
Ethical consideration: We ensured we mentioned confidentiality and anonymity in the process of working on this article.