Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Tomislav Stjepic
Polipraxis Permanence, Kornhausstrasse 3, 9000 St Gallen, Switzerland.
Email: tomislav.stjepic@live.com
Received: Aug 26, 2025 Accepted: Sep 08, 2025 Published: Sep 15, 2025
Citation: Driever L, Stjepic T, Osterwalder J. A common clinical challenge: Cervical lymphadenopathy with fever – what should we look out for? A case report. Ann Case Rep Med Images. 2025; 2(2): 1038.
Copyright: Stjepic T et al. © All rights are reserved
Isolated cervical lymphadenopathy with fever is a common reason for consultation in primary care. A straightforward, practitioner-focused diagnostic pathway is largely lacking in literature. Unlike hospital medicine—where rapid certainty and access to extensive, costly diagnostics is the norm— primary care requires a stepwise approach shaped by clinical evolution. We summarize the diagnostic journey of a patient with lymphadenitis, fever, and malaise, and present a simple, structured, not yet validated algorithm to help distinguish simple reactive cervical lymphadenitis from specific infections, malignancies or chronic granulomatous diseases. A particular focus is given to glandular tularemia, a rare but increasingly important differential diagnosis in Switzerland and other European countries.
Keywords: Cervical lymphadenopathy; Ultrasound; Algorithm; Francisella tularensis.
In mid-August 2021, a previously healthy 37-year-old woman presented to her General Practitioner (GP) with a sudden onset of high fever, chills, profuse sweating, and sore throat. Ultrasound revealed bilaterally enlarged submandibular lymph nodes as the probable cause of sore throat. ENT and general examination were otherwise unremarkable, except for a small aphthous lesion in the pharynx.
Based primarily on the medical history and clinical findings, a bacterial origin, a specific systemic infection, a chronic granulomatous inflammation, and a tumor were ruled out. The working hypothesis, based on experience in a general practice setting in Switzerland, and typical observations in such cases, was viral lymphadenitis. Therefore, further investigations were initially omitted, and a follow-up appointment was scheduled.
Initial phase (Mid-August 2021): The oligosymptomatic patient was initially managed symptomatically with NSAIDs (Ibu-profen 400 mg 3x daily) and oropharyngeal therapeutics (cetylpyridinium chloride, lidocaine hydrochloride, levomenthol, and hexetidine).
Intermediate phase (early September 2021)
Fever returned, with worsening malaise and a papular rash on the abdomen and legs. Submandibular lymph nodes increased in size. Blood tests showed mild leukocytosis and slightly elevated CRP. Assuming a bacterial origin, a 6-day trial of Amoxicillin-Clavulanic Acid normalized lab values but did not relieve lymphadenopathy or fatigue.
Advanced stage (mid to late September 2021): ENT referral and later hospital admission
Ultrasound performed by the GP in mid-September revealed lymph nodes measuring up to 34 × 16 mm, which were echo lucent and partially well-demarcated (Figure 1). ENT consultation some days later confirmed reactive lymphadenitis, and recommended observation. However, the patient and the GP became concerned due to clinical progression.
After six days of inpatient care, patient was discharged in good condition. Infectious disease specialists recommended extending antibiotics to six weeks due to protracted course and relapse risk (up to 15%). Treatment was well tolerated.
As a lesson from this case, a not yet validated structured diagnostic algorithm for ultrasound-confirmed cervical lymphadenopathy accompanied by fever and malaise is proposed early in the clinical presentation of such patients (Figure 2), with ultrasound serving as a key and primary diagnostic tool in the workup.
The approach begins with the exclusion of ENT infections and tumors, followed by a detailed history and evaluation for systemic or specific infection, granulomatous inflammation, or lymph node malignancy when suggested by the ultrasound findings.
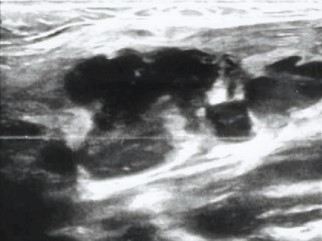
Figure 1: Ultrasound image of an enlarged submandibular lymph node, hypoechoic, polycyclic, well-demarcated, with echogenic surrounding tissue — consistent with reactive lymphadenitis.
Given the GP’s concerns regarding the extent of the ENT assessment, he subsequently conducted a new detailed medical history to enable a more comprehensive evaluation of the patient’s condition. She reported a recent visit to an animal park with contact with goats, residence near a forested area, and frequent insect bites during the summer months. Notably, no tick exposure was recalled. Combined with the rash in week two, this led to suspected tularemia from inhaled contaminated dust or aerosols. Other differentials such as e.g. TB, diphtheria, HIV, and lymphoma were considered unlikely.
Consequently, targeted serological testing, including assays for Borrelia and tularemia, was promptly initiated on September 15. Because of delayed results, a fine needle aspiration (September 22) with pus sampling, PCR for tularemia, and cytology was performed. Due to swelling and increased inflammation, the patient was admitted to hospital on September 23.
Laboratory diagnostics
Hospital admission on September 23rd included comprehensive infectious serology, with repeated testing for tularemia. ENT endoscopy was normal. CT showed cervical abscessed lymphadenopathy (levels II/III). September 15 revealed:
− Serology: High Francisella tularensis titers (IgG >300 U/ mL, IgM>177 U/mL; normal<10 U/mL), negative Borrelia IgM.
− PCR: Positive for F. tularensis.
Hospital serology dated September 22 confirmed: F. tularensis IgG and IgM both markedly elevated, indicating a recent infection.
Hospital measures, clinical course, and discharge
Initial treatment: Upon admission to the hospital IV ciprofloxacin (750 mg BID) was immediately started considering the strong clinical suspicion of tularemia.
Surgery: Cervicotomy with abscess incision performed next day for drainage and sampling. Histology later revealed granulomatous-necrotizing, abscessed lymphadenitis.
Therapy adjustment: Patient had a Grade I anaphylactic reaction to ciprofloxacin. Switched to doxycycline (100 mg BID), leading to rapid improvement.
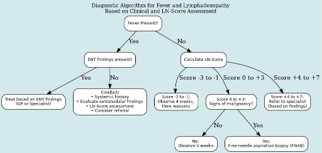
Figure 2: Simple diagnostic algorithm for fever and lymphadenopathy, based on clinical and LN-score assessment.
A Lymph Node Score (Table 1) and malignancy criteria (Table 2) guide further decisions: observation for low scores, fine needle aspiration if malignancy is suspected, or referral to specialists in case of suspicion of a systemic disease, specific infection, chronic granulomatous inflammation or presence of extra nodular findings.
| Parameter | Points |
|---|---|
| Age < 30 years | –1 point |
| Lymph node size < 1.5 cm | –1 point |
| Painful lymph node | –1 point |
| Supraclavicular location | +1 point |
| Firm or hard consistency | +1 point |
| No pain | +1 point |
| Size > 2 cm | +2 points |
| Progressive enlargement | +2 points |
Score interpretation
− –3 to –1: Low risk — observation
− 0 to +3: Moderate risk — monitor vs biopsy based on red flags
− +4 to +7: High risk — specialist referral and workup
| Clinical feature | Suggestive of malignancy? |
|---|---|
| Lymph node size >2 cm | Yes |
| Firm, rubbery, or hard consistency | Yes |
| Non-tender (painless) | Yes |
| Fixed to underlying tissue (non-mobile) | Yes |
| Supraclavicular or epitrochlear location | Yes |
| Persistent enlargement >4–6 weeks | Yes |
| Systemic symptoms (fever, night sweats, weight loss) | Yes ("B symptoms") |
| Rapid growth | Yes |
| Age >40 | Consider higher suspicion |
| Generalized lymphadenopathy | Sometimes (especially lymphoma) |
| Associated hepatosplenomegaly | Yes (esp. hematologic malignancies) |
| Inflammatory signs (redness, warmth, pain) | No (suggests infection) |
Structured diagnostic approach: Cervical swelling requires initial sonography. Identified lymph nodes should trigger structured evaluation. Our proposed algorithm (Figure 1) is based on clinical experience and helps distinguish benign from serious causes.
Our patient had no extraglandular findings (e.g., thyroid disease). Malignancy or granulomatous disease was unlikely. Initial antibiotic trial failed. In-depth history including animal/tick contact, rural exposure, and travel was essential. The combination of environmental exposure, rash, and antibiotic resistance suggested tularemia. The final diagnosis was glandular tularemia.
Delayed serology follow-up and lack of early infectious disease consultation caused a two-week treatment delay, leading to lymph node abscess and hospitalization.
Rising importance of tularemia
Tularemia (rabbit fever) is a rare but notifiable zoonosis in Switzerland, with rising incidence. In 2018, 121 cases were recorded. From 2005–2013: 61 cases. From 2014–2022: 430 cases—a sevenfold increase. Neighboring countries, Sweden, and Finland report similar trends.
The disease is caused by the highly infectious, gram-negative, non-spore-forming bacterium Francisella tularensis. It survives for weeks in moist soil, water, or carcasses but is heat-sensitive. In Switzerland, the less virulent subspecies F. tularensis holarctica predominates.
Transmission: via tick/insect bites, contact with infected animals, contaminated dust/water. In 2021, 41.9% of Swiss cases had vector exposure; 30.3% had contact with wild animals/farm environments.
Incubation: 3–5 days (range 1–21).
Clinical forms: Ulceroglandular and glandular (most common), followed by oculoglandular, oropharyngeal, pneumonic, and typhoidal. Swiss pediatric study: 95% had ulceroglandular or glandular forms. Symptoms include:
Annals of Case Reports and Medical Images
− Fever, chills, headache, fatigue, anorexia, muscle pain, cough, sore throat, GI upset.
Diagnosis: serologic testing after 1–2 weeks of symptoms. Treatment of choice: ciprofloxacin or doxycycline for 14–21 days.
This case illustrates the importance of structured, stepwise and broad differential diagnostics in persistent cervical lymphadenopathy with fever. Particularly in Europe, tularemia should be considered in unclear progressive lymphadenitis cases unresponsive to initial treatment, especially antibiotics. Early diagnosis and appropriate antibiotic treatment can greatly improve outcomes and help avoid complications caused by diagnostic delays. Such delays may lead to serious issues like abscess formation, requiring hospitalization, CT scans, surgical abscess evacuation, and delayed healing.
With rising incidence in Switzerland and other European countries, clinicians should obtain a detailed exposure history, including potential contact with tularemia, and test for tularemia when it is suspected. Our diagnostic algorithm may help distinguish self-limiting conditions from serious and specific differentials, including tularemia.
Patient perspective: The patient reported the long wait for diagnosis as exhausting and distressing. Uncertainty was particularly stressful. Once a likely infectious (not malignant) cause was confirmed, she felt relieved. After diagnosis and effective treatment, she finally saw the ‘light at the end of the tunnel.
Patient consent: The patient granted permission to publish this anonymized case report. The signed consent form is documented in the patient record.