Article Type: Case Series, Volume 2 Issue 2
*Corresponding author: Jian Jing
Department of Pathology, University of Colorado School of Medicine, 12605 East 16th Avenue, Aurora, CO 80045, USA.
Email: Jian.Jing@cuanschutz.edu
Received: Jul 17, 2025 Accepted: Aug 15, 2025 Published: Aug 22, 2025
Citation: Rousselot AL, Jing J. Histologic diagnostic features of echinococcosis in clinical practice. Ann Case Rep Med Images. 2025; 2(2): 1035.
Copyright: Jing J et al. © All rights are reserved
Echinococcosis is a zoonotic parasitic disease caused by Echinococcus tapeworms, leading to the development of hydatid cysts, most commonly affecting the liver and lungs. Clinical manifestations are often nonspecific, making diagnosis challenging. Although rare in the United States, echinococcosis should remain a key consideration in patients with a history of travel to or immigration from endemic regions, the details can be overlooked in initial evaluation [1]. In routine practice, cystic lesions detected on imaging are commonly biopsied to establish a definitive diagnosis [2].
We describe two cases in which pulmonary and hepatic cysts were incidentally discovered during imaging performed for unrelated clinical concerns. This report emphasizes the pathological features observed in small biopsy specimens that are indicative of echinococcosis. A retrospective review of both patients’ travel histories revealed prior residence in or travel to endemic areas, and subsequent serologic testing confirmed Echinococcus granulosus infection.
Echinococcosis is a zoonotic parasitic infection caused by the larval stages of Echinococcus tapeworms. It affects individuals of all ages and is globally distributed, forming cystic lesions most commonly in the liver and lungs (hydatid cysts). It remains an important diagnostic consideration in patients from endemic regions, especially those with occupational exposure to livestock such as sheep or goats [1].
Several Echinococcus species are pathogenic to humans, with the two most clinically relevant being:
Echinococcus granulosus – Causes unilocular hydatid cysts. Dogs serve as definitive hosts, while sheep, goats, and other ungulates act as intermediate hosts. Humans become accidental intermediate hosts through ingestion of eggs. Grossly, cysts are large, spherical, often with a fibrous outer rim and internal daughter cysts. This form is globally distributed and the most common cause of human echinococcosis.
Echinococcus multilocularis – Causes alveolar echinococcosis, characterized by multilocular cystic lesions with central necrosis and fibrous margins. Red foxes are the definitive hosts; rodents are the typical intermediate hosts. This form is more aggressive and locally invasive [3].
In E. granulosus infection, the life cycle begins when the intermediate host ingests eggs via the fecal-oral route. The eggs hatch in the small intestine into six-hooked oncospheres, which penetrate the intestinal wall and disseminate via blood or lymphatics, most commonly to the liver (52-77%) and lungs (10-40%). There, they develop into hydatid cysts, consisting of a germinal layer that produces brood capsules and protoscolices. In humans, these cysts grow slowly and can reach large sizes, often containing liters of fluid and thousands of protoscolices. The cycle is completed when a definitive host (e.g., a dog) ingests these cysts, allowing the protoscolices to mature into adult tapeworms in the intestine [1,3].
Clinically, E. granulosus infections may remain asymptomatic for years. Symptoms arise due to cyst enlargement or rupture, leading to mass effect or complications such as biliary obstruction, secondary infection, or peritonitis. Pulmonary cyst rupture may cause pleuritis, pneumothorax, or respiratory symptoms. Systemic effects including eosinophilia, fever, or even anaphylaxis may occur if cyst contents leak into surrounding tissues [4,5].
The diagnostic evaluation of echinococcosis typically begins with imaging. Ultrasonography is considered the gold standard, particularly for hepatic lesions, while Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) provide additional anatomical detail and are useful for both hepatic and pulmonary involvement [4].
Serologic testing plays a key role in confirming the diagnosis. Enzyme-Linked Immunosorbent Assay (ELISA) and immunoelectrophoresis are commonly used to detect antibodies against Echinococcus species. Immunoblot assays may further confirm the presence of echinococcal antigens and help distinguish species [2].
Although not essential for diagnosis, histopathologic examination can provide definitive support—particularly when imaging and serology are inconclusive [6]. Characteristic microscopic features include the presence of protoscolices, hooklets, or abundant laminated membranes. Grossly, resected hydatid cysts are typically spherical, unilocular, and thick-walled, often containing internal daughter cysts. Cysts can grow to sizes of up to 30 cm in diameter [6,9].
Histologically, the cyst wall generally displays three to four distinct layers:
1. A thick, outer, acellular laminated membrane
2. A cellular germinal layer with a transparent, nucleated lining
3. Protoscolices budding from brood capsules within the germinal layer with/without suckers and birefringent hooklets
4. An additional outer fibrous layer may be present, indicating a host granulomatous or granulation tissue reaction. However, such host responses are less pronounced in echinococcal infections compared to other parasitic or infectious etiologies [6,7].
Treatment options for echinococcosis range from pharmacologic therapy to surgical intervention. Benzimidazole compounds (e.g., albendazole or mebendazole) are commonly used. However, surgical resection remains the mainstay of treatment, especially for pulmonary hydatid disease, where complete excision is often necessary for cure [8,9].
In hepatic disease, the PAIR technique (puncture, aspiration, injection of a scolicidal agent, and re-aspiration) offers a minimally invasive alternative. Scolicidal agents may include hypertonic saline (20%), alcohol (95%), cetrimide, or povidoneiodine. This method is generally not recommended for pulmonary cysts due to the increased risk of cyst rupture, which can lead to complications such as hemoptysis or life-threatening anaphylaxis [5,9,10].
Case #1: A 40-year-old from Bolivia presented with right lower quadrant abdominal pain, nausea, and vomiting. A physical exam showed a positive Rovsing sign and an elevated white blood count. She was admitted for acute appendicitis, which was supported by a CT scan. However, the CT scan also incidentally demonstrated multiple calcified liver masses, up to 2.6 cm in greatest dimension. Due to concern for malignancy, interventional radiology performed a fine needle aspiration which showed Echinococcus organisms with a background of necrosis and inflammation. She completed treatment with albendazole and has not had any recurrences or complications from Echinococcosis.
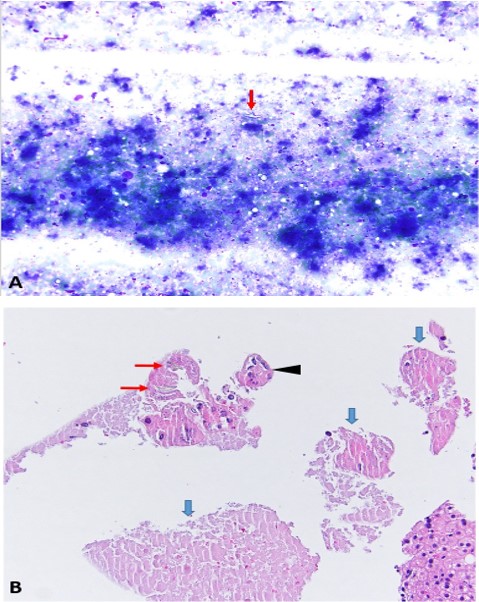
Figure 1: (A) Cytology smear from ROSE reveals a rare, refractile hooklet (red arrow) within an acellular necrotic background. (Diff-Quik, 200×) (B) Cell block highlights three key histologic components: laminated membrane (blue arrow) and protoscoleces (black arrowhead) (H&E, 200×).
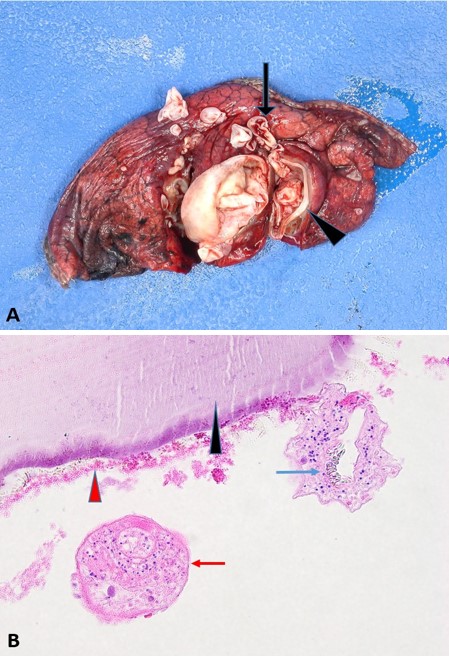
Figure 2: (A) Gross specimen demonstrating the fibrous cyst wall (arrowhead) and multiple daughter cysts (arrow). (B) Histologic section highlighting key components of Echinococcus: laminated membrane (black arrowhead), germinal membrane (red arrow head), hooklets (blue arrow), and protoscoleces (red arrow). (H&E, 400×).
Case #2: A 57-year-old from Peru with a history of sheepherding and recent pruritus, emesis, hemoptysis, and self-limited flushing, noted after falling off a horse. Computed Tomography (CT) scan showed pulmonary cysts in the right and left lower lobes as well as “water-lily sign” demonstrating collapsed cyst wall. Labs showed increased eosinophilia up to 2.4×106 (reference range: 0.0 0.4×106) and positive serum Echinococcus IgG. Right lower lobe wedge resection confirmed organisms consistent with Echinococcus infection. He was admitted for further surgery three weeks later which showed left upper and lower lobe with Echinococcus infection. He was treated with albendazole, but his course was complicated by pneumothorax, bilateral deep venous thrombi, pain, bronchopleural fistulas, and elevated liver function tests. After a difficult hospital stay, he improved; his last imaging report noted no findings concerning for infection.
Echinococcosis, most commonly caused by Echinococcus granulosus, is a parasitic infection that primarily affects the liver and lungs. Although rare in the United States, it should remain in the differential diagnosis for patients from endemic areas or with a history of exposure to livestock, particularly sheep and goats [1]. Diagnosis can be especially challenging in patients presenting with nonspecific symptoms or when the clinical history is incomplete.
In routine practice, these lesions may first present during cytology Rapid On-Site Evaluations (ROSE). Due to the cystic nature of the lesions and the typically scant cytologic material, key diagnostic elements can be overlooked, resulting in delays in diagnosis and treatment [9,10]. This was evident in Case 1, where the initial smear was reported as negative for malignant cells. Upon closer review, rare refractile hooklets were identified in a background of abundant acellular necrotic debris a nonspecific finding, but one that is more commonly observed in cytology smears of echinococcosis. Similarly, cell block analysis must be carefully reviewed, as the diagnostic parasitic structures may be sparse and embedded within the surrounding unremarkable tissue.
Case 2 represents a more classic presentation, with consistent clinical, radiologic, and pathologic findings. This case highlights the full spectrum of echinococcal disease and underscores the importance of recognizing key diagnostic features, particularly in small biopsy specimens with limited tissue. In contrast, Case 1 illustrates how subtle but definitive findings when paired with retrospective clinical correlation can lead to timely diagnosis and appropriate treatment. Together, these two cases exemplify the diagnostic challenges and learning opportunities inherent in the workup of echinococcal disease.
These cases emphasize the critical importance of early recognition and diagnosis of echinococcosis. While classic presentations may offer more straightforward diagnostic pathways, many cases are subtle, with key cytologic or histologic features easily overlooked especially in the absence of detailed clinical histories. A high index of suspicion, thorough morphologic review, and thoughtful clinicopathologic correlation are essential to avoid delayed diagnosis and minimize complications such as extended hospitalization, invasive surgeries, and disease progression.