Article Type: Case Series, Volume 2 Issue 2
*Corresponding author: Jordanne Nichols
College of Osteopathic Medicine, Department of Biomedical Science Rocky Vista University, Colorado, 8401 S Chambers Road, Parker, CO 80112, USA.
Email: Jordane.nichols@co.rvu.edu
Received: Jul 12, 2025 Accepted: Aug 12, 2025 Published: Aug 19, 2025
Citation: Nichols J, Grant-Kirschke V, Bolen R, Grorge I. Depression as primary symptom presentation of glioblastoma multiforme: A case series. Ann Case Rep Med Images. 2025; 2(2): 1034.
Copyright: Nichols J et al. © All rights are reserved
Glioblastoma Multiforme (GBM), a subclass of astrocytoma, is widely recognized as the most aggressive form of neurologic tumors [1]. Astrocytomas that subsequently have increased microvascular proliferation and/or necrosis present within the tumor are classified by the World Health Organization (WHO) as stage IV astrocytomas, synonymous with GBM or simply glioblastoma [1]. Although different in designation, the terms stage IV astrocytoma, GBM, and glioblastoma are all accepted as nomenclature for GBM and are commonly used interchangeably. Due to the abnormal cytology and proliferative nature of grade IV astrocytomas, prognosis is poor and often fatal [1].
Both primary and secondary glioblastomas commonly present with symptoms such as headaches, cognitive impairments, and seizures, though the manifestation of these symptoms can vary among patients. A previous study analyzing symptom presentation in patients with primary and secondary brain tumors between 2000 and 2014 found that symptoms of seizures, weakness, and confusion were highly correlated with Central Nervous System (CNS) tumor diagnosis (excluding meningiomas) [2]. Of the 8,184 study subjects, 438 had depression (5%) compared to 699 subjects out of the 28,110 control patients (2%) [2]. Additionally, cognitive impairments, such as an inability to concentrate or generalized confusion, were more prevalent in the study group (5%) than in the control group (0.03%) [2]. While this study highlights the difference between the presence of cognitive impairments in the study group and negative control, it fails to address the significance of this finding clinically.
As a multifactorial disease, depression can present in numerous ways including lack of concentration, fatigue, and disorientation. Specifically, in the age cohort of 40 to 64 years, depression can be particularly nuanced, with symptoms not always aligning with stereotypical manifestations [3]. This period of adulthood often brings forth a range of significant life transitions, including career changes, family dynamics, and personal adjustments, making accurate diagnosis and intervention clinically challenging. Depression is characterized by a spectrum of symptoms that extend beyond the emotional sphere. Cognitive difficulties, such as decreased concentration and memory problems, can easily be mistaken for routine stress or age-related changes [3]. Fatigue, sleep disturbances, and changes in appetite, which often accompany depression, could be disregarded as mere lifestyle adjustments during this stage of life [3]. This case series emphasizes the importance of primary care providers and mental health counselors recognizing these subtleties and considering their potential connection to underlying medical conditions.
Three previously published case studies were carefully selected for inclusion in this case series based on specific criteria. The inclusion criteria focused on patients diagnosed with primary GBM through radiographic imaging, with initial symptom presentation available for review. Exclusion criteria included previous history of mental illness, including non-situational depression, comorbid oncologic conditions, and patients outside of the age range of 46-64.
The case series consists of two male sex patients and one female sex patient, with no denotation of other gender preference/orientation. Each case was thoroughly analyzed based on the patients’ initial symptom presentations prior to their GBM diagnosis. Due to the deidentification of the patient’s identity through the conservation of medical number, name, and identifying factors, a HIPAA exemption was granted following the direction of Rocky Vista University Institutional Review Board (IRB).
A 46-year-old male was admitted to the emergency department due to perceived psychiatric failure to thrive. The patient, who was seeing a psychiatrist for newly onset depression, was prescribed Duloxetine and Bupropion to manage the symptoms. However, both medications were unsuccessful in alleviating the patient’s depression. Symptoms reported by the patient included irritability, decreased concentration, recurrent headaches, weight loss, and decreased motivation to care for himself. The patient was admitted to the hospital with the diagnosis of depression and associated psychosis. During the patients stay under psychiatric evaluation, decreased expression of emotions, nonverbal behavior, and decreased movement was noted. Blood analysis while in the hospital revealed hypernatremia with no other significant findings and therefore the patient was transferred out of the psychiatric department to general medicine for treatment of suspected dehydration. Neurologic testing under the general medical service revealed decreased appreciation of painful stimuli on the right compared to the left, decreased reflexes on the right, as well as inability to ambulate the right side of his body. An MRI (Figure 1) was ordered reflecting a large mass in the left frontal lobe infiltrating the corpus callosum. The tumor had characteristics histologically compatible with a GBM in the company of necrosis. The patient was put under palliative care and died one week later [4].
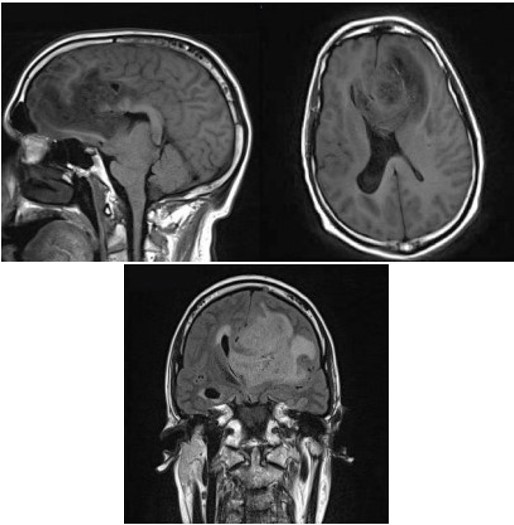
Figure 1: (Adapted from Figure 1 of. Leo RJ, Frodey JN, Ruggieri, 2020) Magnetic resonance imaging of a glioblastoma in the left frontal lobe infiltrating through the corpus callosum with mass effect imposing on the ventricles.
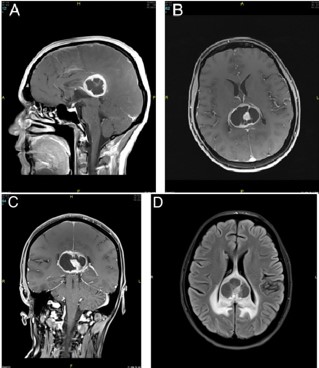
Figure 2: (Adapted from Figure 1 of Hale YapIci-Eser et al., 2016) GBM within the splenium of the corpus callosum with associated cerebral edema.
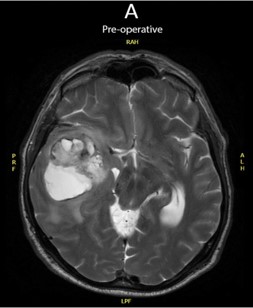
Figure 3: (Adapted from Figure 1 of Franssen and Sienaert, 2018) MRI of a GBM in the right temporal lobe resulting in herniation of the uncus and displacement of surrounding tissue.
A 46-year-old woman presents with a 6-month history of inability to experience pleasure, fatigue, and decreased motivation. She had noticed a change in her personality from extroverted to more introverted while denying any triggering life event. The patient also stated that she had decreased concentration, hypersomnia, and associated her symptoms with feeling depressed. She had a history of a single depressive episode two years prior due to an isolated stressor that resolved after two months with antidepressant treatment, at which time she discontinued her medication and had not experienced any similar episodes. Patient denied headaches, hallucinations, or suicidal ideations. Testing showed impairments with visual and primary verbal memory testing, which resulted in the ordering of an MRI with contrast of the brain. The MRI (Figure 2) revealed a cystic mass as well as associated edema in the posterior corpus callosum which was histologically classified with a biopsy as a GBM. The tumor was removed, and the patient was discharged five days following the resection of the GBM [5].
A 57-year-old male was brought to the emergency department due to declining symptoms of a depressive event. The patient was experiencing weight loss, decreased ability to care for himself, nocturnal urinary incontinence, and increased introversion. Upon presentation the patient had an apathetic demeanor with delayed, fragmented, and repetitive speech. He also was unable to sustain balance although he had hyperactive motor response in locations such as his jaw and extremities. Patient had no previous history of mental health disorders. The patient was admitted to the psychiatric department of the hospital with the diagnosis of a depressive episode with catatonia. In the psychiatric ward the patient was given 1 mg of lorazepam four times daily which improved the patient’s clinical symptoms. During admission the patient’s behavior altered towards inappropriate sexual conduct, aggression, increased impulsivity, as well as diplopia. A neurological exam was done that found slow twisting movements of the right distal extremities (athetoid movements). An MRI was ordered revealing a pressing necrotic mass in the right temporal lobe causing herniation of the uncus. Histological analysis following transection of the tumor reflected a GBM which was successfully treated with removal followed by radiation and chemotherapy. One year following GBM treatment the patient had new onset symptoms of anxiety and seizures. With neurological follow up it was determined that the GBM had recurred in the frontal portion of the temporal lobe and the patient died 4 months later [6].
| Case | Symptom presentation | Diagnosis on hospital admission | Final decision for imaging | Location of brain tumor |
|---|---|---|---|---|
| Case 1 | Depression | Depression with Psychotic features | Unequal bilateral reflexes | Left Frontal Lobe |
| Failed pharmacologic treatment for depression | Unresponsive to painful stimuli on the right side of the body | Genu of corpus Callosum infiltration | ||
| Increased irritability | Ventricular effacement | |||
| Decreased motivation | ||||
| Recurrent headaches | ||||
| Case 2 | Fatigue | Not disclosed in case | Primary verbal and visual memory impairment | Posterior corpus callosum |
| Avolition | Associated edema in adjacent periventricular white matter | |||
| Depression | ||||
| Decreased concentration | ||||
| Hypersomnia | ||||
| Case 3 | Depression | Depressive episode with catatonia | Double vision | Right temporal lobe with uncal herniation |
| Deterioration of a depressive episode | Abnormal electroencephalogram | |||
| Weight loss |
| Case | Gender | Age | Location of case publication | Year of Case Publication |
|---|---|---|---|---|
| Case 1 | Male | 46 | New York, USA | 2020 |
| Case 2 | Female | 46 | Istanbul, Turkey | 2016 |
| Case 3 | Male | 57 | Kortenburg, Belgium | 2018 |
Disease presentation in the central nervous system is complex and variable. Important considerations of symptom presentation include tumor location, size, and composition [7]. In the three cases of this series, case one and two share tumor infiltration into the corpus callosum reflecting a possible correlation between symptom presentation. Previously published studies on infarctions within the corpus callosum show symptoms related to interhemispheric disconnection, though manifestations in this region are often vague [7]. This can be compared to frontal lobe involvement in which ‘frontal lobe syndrome’ may be noted with behavioral changes and decreased cognitive executive functions [8]. While it may seem that depression correlated with disease presentation should always involve a lesion in the frontal lobe, this is proven within analysis of the cases to be untrue. Therefore, if the location of the brain lesion does not strongly correlate with psychiatric manifestations of disease, why are clinicians not trained to recognize these symptoms as possible presentations of a central malignant state?.
This may be attributed to the complex nature of depression presentation as well as concurring comorbidities. Depression for those in the 40-64 age group often presents with symptoms such as persistent sadness, loss of interest in enjoyable activities, changes in appetite and sleep, as well as difficulty concentrating, and recurrent thoughts of death or suicide [3]. This age group might also experience certain unique aspects, such as the onset of depression coinciding with ‘midlife crises’ or life transitions (e.g., empty nest syndrome) [3]. Individuals in this specified age bracket may be undergoing numerous life adjustments including career changes or retirement, physical health changes, and shifts in family dynamics [3]. These transitions can be stressful and may trigger or exacerbate depressive symptoms.
Furthermore, a study published in the New England Journal of Medicine illustrates how depression in older adults, including those in their late middle age, is often associated with coexisting medical illness and cognitive dysfunction, complicating the clinical presentation and treatment of depression [9]. This underscores the need of heightened attention for patients of this age range presenting with new onset symptoms of depression, potentially requiring more extensive workups. However, how is the need for advanced testing addressed when patients self-refer to psychologists for their perceived depression, given that these professionals typically lack the authority to order such tests?
Self-sought treatment for depression most commonly includes Cognitive Behavioral Therapy (CBT), which has been found to be as effective as pharmacotherapy for depression, with benefits that may last longer for some patients [10]. Currently, patients are able to access psychologists on a self-referral basis for counseling and CBT resources, which increases access to care for patients, but may be harmful for patients experiencing the perceived depression when in reality there is a more serious physiologic process occurring. Interdisciplinary communication between psychologists and physicians when patients present with abnormal or persistent mental health conditions is key to filling this care gap. This potentially could create more comprehensive care even for patients even without malignancy as studies have shown that the combination of psychotherapy and pharmacotherapy tends to be more effective than either treatment alone [11].
Depression symptom presentation in isolation from malignancy can be complex, including cognitive dysfunction masked as numerous medical ailments including endocrine, neurologic, or even physiologic [12]. Cognitive dysfunction in depression, similar to that observed in patients with brain tumors, can encompass memory attention, executive function and processing speed. As noted by Kaser, Zaman, and Sahakian, neurocognitive deficits tend to persist even after mood symptoms recover [12]. Moreover, MacQueen and Memedovich discuss that cognitive impairment is associated with poor overall functional outcomes in Major Depressive Disorder (MDD), paralleling the cognitive challenges faced by patients with brain tumors [13]. Neurologic testing performed by a physician in conjunction with increased communication could help to elevate the standard of care and differentiate these presentations.
Primary care physicians, who manage roughly 80% of antidepressant medications and 60% of patients with depressive symptoms, play a crucial role in screening and treatment of depression [14]. The American Academy of Family Physicians (AAFP) recommends screening for depression with a PHQ-9 questionnaire and treating accordingly to improve quality of life and prevent adverse events such as suicide [15]. Within this guideline, lab work is suggested forolder populations to rule out conditions that may mimic depression such as electrolyte imbalances or thyroid disorders, but there is no mention of potential neurological risks or associations [15]. This can be differentiated from a study published by the Indian Journal of Psychiatry within the National Library of Medicine stating that further investigation, including neuroimaging, should be indicated in patients with new onset depression at advanced age, those resistant to pharmacologic treatment, as well as neurologic expression in conjunction with symptoms of depression [16].
In this case series, all three patients did not receive immediate neurologic testing or MRI until symptoms had advanced, resulting in a delay of care that could have been prognostically substantial. This may be due to different standards based on geography and resources in locations such as India compared to the United States, Belgium, or Turkey, fear of over diagnosing, or care of depression by primary care physicians who are overburdened with patient conditions. Neuroimaging may be delayed or not ordered when a physician is unsure of its definitive benefit due to cost burden on the patient and potential concern of unnecessarily over diagnosing asymptomatic conditions. According to NH Health Cost, an MRI of the brain can cost a patient between $500-$9,000 dollars [17]. This can be a significant financial burden and therefore cannot be abundantly ordered and may even be deferred by some physicians. Until payment load decreases for patients, neuroimaging will most likely continue to be postponed by physicians until symptoms are of extreme concern. In medical school, it is taught that “what is common, is common”, and “think horses when you hear hooves, not zebras”, and most of the time this is probably true when it comes to patients with depression due to its extreme prevalence. The number of incident cases of depression worldwide increased from 172 million in 1990 to 258 million in 2017, an increase of 49.86% [18]. Therefore, with this advanced quantity of depression within the population it is important to recognize that while neurologic malignancy may not be a common cause of perceived depression by a patient, it is still an important consideration. These cases did not specify the type of physician or care initially sought for depressive symptoms or whether neurologic exams were included with their visit, but the cases did reveal that they were diagnosed and treated as if they had depression until their diseased state progressed to such a level that they required more critical care. This caused delays in diagnosis and reduced the time these patients had to spend with their loved ones, given the inevitable and severe nature of their prognosis.
Limitations of this study include utilizing only three previously published cases regarding the symptom of depression for patients with glioblastomas. Due to this decreased sample size and particular symptom, this does not create definitive correlation between depression as a symptom of glioblastoma multiforme. In addition, many previously published cases reflect the presentation with other psychiatric disturbances, but depression was isolated to keep the cases homogenous. More studies and surveys need to be conducted to understand the depth of correlation between patients with glioblastoma who experience depression as a disease manifestation prior to the knowledge of their diagnosis. Furthermore, standards need to be re-evaluated for psychologists, family practice physicians and psychiatrists when confronted with an older patient experiencing treatment resistant depression or sudden onset of depression.
Education on the correlation between new onset depression in the middle to older aged population and neurologic oncology is crucial for ensuring high-quality care. Neurological physical exams are quick and comprehensive ways to ensure that patients being diagnosed and treated for depression are being examined properly and proactively. Furthermore, patient access to physician care and imaging is a vital element in ensuring timely diagnosis and treatment.
Declarations: This research was presented as a poster presentation at the American Academy of Neurology’s annual conference on April 16th, 2024.