Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Luca Zazzeron
Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital and Harvard Medical School, Boston, MA 02114, 55 Fruit St. Boston, MA, 02114, Thier Building room 505, USA.
Email: lzazzeron@mgb.org
Received: Jul 16, 2025 Accepted: Aug 06, 2025 Published: Aug 13, 2025
Citation: Suriani RJ, Zazzeron L. Anesthetic management of a patient with hypertrophic cardiomyopathy on mavacamten. Ann Case Rep Med Images. 2025; 2(2): 1032.
Copyright: Zazzeron L et al. © All rights are reserved
Hypertrophic cardiomyopathy (HCM) is characterized by asymmetric Left Ventricular (LV) hypertrophy, resulting in a dynamic LV Outflow Tract (LVOT) obstruction that can cause hemodynamic collapse. While HCM treatment has traditionally involved pharmacologic rate control and in severe cases, surgical intervention, Mavacamten, a cardiac myosin ATPase inhibitor which effectively reduces myocardial contractility, has emerged as a novel treatment that significantly reduces LVOT gradients and improves exercise tolerance. Anesthetic management of patients with HCM is challenging, as anesthetic drugs can depress cardiac contractility and many situations encountered during surgery can worsen LVOT obstruction. The effects of Mavacamten (a negative inotropic drug) on intraoperative hemodynamics and anesthetic outcomes has not yet been studied. We describe the anesthetic management of a patient with HCM treated with Mavacamten undergoing two separate urologic procedures. Despite the concurrent use of a negative inotropic drug, the patient remained hemodynamically stable throughout the surgical procedures. More studies will be needed to determine the safety of various anesthetic techniques in patients on Mavacamten with varying degrees of LV dysfunction.
Keywords: Hypertrophic cardiomyopathy; Mavacamten; Heart failure; Anesthesia.
Abbreviations: HCM: Hypertrophic Cardiomyopathy; LV: Left Ventricle; LVOT: Left Ventricle Outflow Tract; BMI: Body Mass Index; EEG: Electroencephalogram; TTE: Trans-thoracic Echocardiography.
HCM is the most common genetic heart disease worldwide, characterized by asymmetric LV hypertrophy, impaired relaxation, and hyperdynamic contractility [1]. The septal hypertrophy causes Left Ventricle Outflow Tract (LVOT) narrowing. The diagnosis of HCM is made by doppler echocardiography, with peak LVOT pressure gradient determining the degree of obstruction (<30 mmHg mild, 30-50 mmHg moderate, >50 mmHg severe). Treatment of HCM involves pharmacologic measures (typically beta blockers) and sometimes surgical intervention (alcohol septal ablation, surgical myomectomy).
Anesthetic management of patients with HCM can be challenging. Hemodynamic goals in HCM include maintenance of preload, afterload, sinus rhythm, and negative chronotropy, all of which avoid exacerbation of LVOT obstruction [2]. These considerations are particularly relevant during induction of anesthesia, when reduced afterload from vasoplegic agents or sympathetic stimulation and tachycardia from laryngoscopy can worsen obstruction and cause hemodynamic instability. Furthermore, positive pressure ventilation, abdominal insuflation, and reverse Trendelenburg positioning all result in preload reduction. It is therefore essential to maintain favorable hemodynamic conditions throughout the anesthetic.
Mavacamten is a new drug that has been recently approved for the treatment of HCM. It is a small molecule that inhibits the cardiac myosin ATPase and normalizes the contraction and relaxation of myocardium [3]. Pre-clinical studies have shown that Mavacamten attenuates cardiac contractility, increasing chamber dimensions while preserving filling pressures [4]. Clinical studies have demonstrated a significant decline in LVOT gradient as well as improvement in exercise capacity relative to placebo [5]. These results demonstrate numerous hemodynamic benefits to HCM patients. However, there is currently no literature describing the management of patients taking Mavacamten undergoing anesthesia. As this medication becomes more frequently prescribed, it is necessary to understand its implications during anesthesia. We therefore describe the anesthetic courses of a patient with HCM taking Mavacamten while undergoing two urologic surgeries.
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
We describe a case of a 67-year-old male with a BMI of 37.6 and a past medical history of HCM, obstructive sleep apnea, hyperlipidemia and recently diagnosed prostate cancer. During staging he was found to have a renal mass and he was scheduled for robotic laparoscopic partial right nephrectomy.
The patient had a longstanding history of HCM. In July 2022 his symptoms and echographic findings had shown signs of progression. His dyspnea on exertion after climbing one flight of stairs had worsened and the peak LVOT gradient had increased, from 52 mmHg in 2015 to 96 mmHg in July 2022. For this reason he was prescribed Mavacamten 5 mg daily. After 3 months of treatment the peak LVOT gradient had decreased to 36 mmHg at rest and 54 mmHg with Valsalva. The ejection fraction did not decrease significantly and therefore the Mavacamten dose was increased to 10 mg daily. Three months later, in March 2023, the peak LVOT gradient had slightly improved (32 mmHg at rest and 53 mmHg with Valsalva, Figure 1A).
The patient then presented for partial nephrectomy. A preinduction radial arterial line was placed for hemodynamic monitoring. Anesthesia was induced with midazolam 2 mg, fentanyl 100 mcg, etomidate 20 mg, propofol 80 mg, and rocuronium 100 mg. The patient was intubated uneventfully using a video laryngoscope. Phenylephrine infusion was started at 50 mcg/ min at induction then decreased to 20 mcg/min shortly after induction. Anesthesia was maintained with sevoflurane 1%, propofol 50 mcg/kg/min, rocuronium boluses, and dexmedetomidine boluses (20 mcg total). The depth of anesthesia and neuromuscular blockade were assessed with processed EEG and with quantitative train-of-four monitoring respectively. The patient received standard antiemetic medications (dexamethasone 8 mg and ondansetron 4 mg) as well as hydromorphone (1 mg) for analgesia. The patient remained hemodynamically stable for the entirety of the anesthetic (Figure 1B). The surgery was uncomplicated, and the patient was extubated in the operating room uneventfully. He was discharged home on postoperative day 2.
One month after surgery a repeat TTE showed peak LVOT gradient improved to 11 mmHg at rest and 44 mmHg with Valsalva (Figure 1A). The patient then re-presented two months later for open bilateral nerve sparing radical prostatectomy for prostate adenocarcinoma. Standard monitors were utilized without intra-arterial blood pressure monitoring. Intraoperative anesthetic management was otherwise similar to the previous surgery and the patient remained hemodynamically stable without anesthetic complications (Figure 1C). The patient was discharged home on postoperative day 1. One month postoperatively, repeat TTE showed further improvement in peak LVOT gradient to 6 at rest and 9 with Valsalva (Figure 1A).
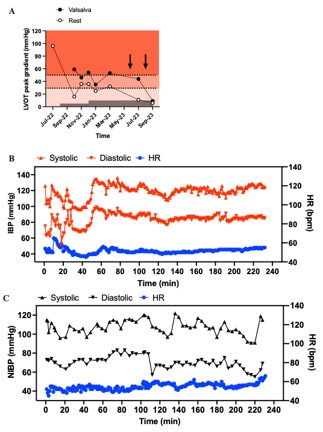
Figure 1: (A) Time course of LVOT peak gradient assessed by transthoracic echocardiography at rest (open circles) or during a Valsalva maneuver (black circles). Red shaded areas and dotted lines represent reference values for mild, moderate or severe degrees of LVOT obstruction. The gray area represents Mavacamten daily dose. Arrows indicate the time of the two surgeries. (B & C) Intraoperative hemodynamic course. IBP: Invasive blood pressure; HR: Heart rate; NIBP: Non-invasive blood pressure.
HCM affects approximately 20 million people worldwide and is defined as increased LV wall thickness >15 mm not solely due to abnormal loading conditions [6]. Genetic causes include mutations in genes encoding myocardial contractile proteins [1]. Symptoms include those of heart failure, such as fatigue and exertional dyspnea, as well as sudden cardiac death, although many patients remain asymptomatic. Symptoms primarily result from LVOT obstruction caused by mitral valve systolic anterior motion. Diagnosis is made via echocardiography or cardiac magnetic resonance imaging. Initial Transthoracic Echocardiographic (TTE) evaluation includes assessment of LVOT gradient at rest, during Valsalva, and while standing, in order to assess for inducible LVOT obstruction defined as LVOT gradient >50 mmHg. Symptomatic patients that do not meet these criteria undergo exercise TTE to further assess for obstruction [7,8].
Management of HCM is multifaceted and dependent on symptoms and obstruction severity. All patients should attempt lifestyle modifications such as dehydration avoidance and weight loss. Patients with symptomatic obstruction are prescribed non-vasodilating beta-blockers such as metoprolol, which both reduce induced LVOT obstruction and improve symptoms. Other medications (dysopyramide, calcium channel blockers) are used if beta blockers are poorly tolerated or ineffective. Surgical procedures such as ventricular septal myomectomy or alcohol septal ablation are reserved for patients with very high LVOT gradients, severe symptoms, or symptoms despite maximal medical therapy. Implantable cardioverter defibrillators are recommended as secondary prevention in patients with a history of cardiac arrest, or as primary prevention in patients with an elevated risk of sudden cardiac death [7].
Recently, Mavacamten has emerged as a novel pharmacotherapy for HCM. Mavacamten is a cardiac myosin ATPase inhibitor that reduces cardiac contractility, thereby stabilizing the otherwise abnormal contractile function of mutant sarcomeres [3]. It gained FDA approval in 2022 and is indicated in patients with symptomatic (NYHA class II-III) HCM. Use is reserved for patients who remain symptomatic despite maximum dose medical therapy. In phase 3 clinical trials, Mavacamten improved symptoms and reduced LVOT gradient compared with placebo in patients with NYHA class II-III heart failure due to HCM [9]. Notably, all enrolled patients had a pre-treatment Left Ventricular Ejection Fraction (LVEF) of at least 55%. A potential risk of Mavacamten therapy is reduction in left ventricular systolic function due to negative inotropy, in this trial seen as a significant but mild mean reduction in LVEF (-3.9%). Six percent of patients had a reduction in LVEF to <50%, although in all cases this was reversible with drug cessation. Mavacamten therefore carries an FDA black box warning addressing the possibility of inducing heart failure [10].
Traditional intraoperative HCM management involves maintaining low LVOT gradient by maintaining preload, afterload, and negative chronotropy. Preload is maintained through fluid administration and avoidance of high tidal volumes or high positive end expiratory pressures during mechanical ventilation. Afterload is maintained through slow titration of anesthetic agents and use of alpha-1 adrenergic agonists (phenylephrine) to increase systemic vascular resistance. Avoidance of betaadrenergic agonists such as epinephrine and norepinephrine prevent positive chronotropy that worsens LVOT obstruction, as does pretreatment of sympathetic stimulation (i.e. laryngoscopy) with beta blockers and opioids [2]. Together these measures improve LV diastolic filling, preventing collapse and obstruction of the LVOT during systole.
Both target and side effects of Mavacamten are relevant to the management of HCM patients undergoing anesthesia. Mavacamten causes a reduction in LVOT gradient over time, which in itself is beneficial in avoiding potentially dangerous hemodynamic consequences resulting from the physiologic stress of anesthesia and surgery. However, the means by which Mavacamten achieves this reduction, namely via myosin inhibition leading to negative inotropy and reduction in LV systolic function, may introduce the risk of heart failure decompensation in such situations. This is especially relevant for patients with baseline low LVEF, as such patients were excluded from phase 3 clinical trials. It is unclear to what extent Mavacamten may reduce systolic function in these patients who are most vulnerable to adverse cardiac events during anesthesia. Therefore, as more of the HCM population is treated with this medication, it is essential to elucidate its effects on anesthetic tolerance. Additionally, it is unclear to what extent Mavacamten’s effects may interact with medications commonly used in anesthesia, such as hypnotics and opioids that elicit varying degrees of cardiodepression and/or vasoplegia, as well as vasoactive medications that directly modulate systemic vascular resistance. At present, there is no literature describing anesthetic management for patients treated with Mavacamten, and it is currently unclear to what extent these patients are able to tolerate general anesthesia.
This case report describes a 67-year-old patient with symptomatic obstructive HCM treated with Mavacamten undergoing general anesthesia for two urologic surgeries. At the time of the first procedure, a robotic partial nephrectomy, he had undergone eight months of Mavacamten treatment with improvement in peak LVOT gradient from 96 mmHg to 53 mmHg. He tolerated the procedure well, including induction with etomidate and propofol, maintenance with sevoflurane and propofol, abdominal insuflation, and emergence/extubation without significant departure from his hemodynamic baseline, utilizing intra-arterial monitoring. Three months later, given the uncomplicated course of his prior anesthetic and further improvement in the peak gradient to 44 mmHg, he underwent open radical prostatectomy without invasive hemodynamic monitoring and he tolerated well this second procedure.
These findings suggest that general anesthesia for both laparoscopic and open abdominopelvic surgery can be well tolerated by patients taking Mavacamten for symptomatic obstructive HCM. Such patients may reasonably undergo anesthetics performed with standard agents and techniques, without necessarily requiring invasive hemodynamic monitoring, if deemed safe and appropriate by the anesthesiologist. Notably, the patient described had a normal Left Ventricular Ejection Fraction (LVEF) both before and during treatment with Mavacamten. Ensuring that LVEF is preserved in patients receiving this medication would be advisable prior to undergoing surgery and anesthesia. More literature is necessary to determine the extent to which these patients may tolerate other types of surgeries and anesthetics. Additional studies are also needed to determine Mavacamten’s effects on patients with reduced LVEF, as well as the ability of these patients to tolerate anesthesia during treatment.
Authors contributions: Robert J Suriani Jr and Luca Zazzeron, collected the data, drafted, reviewed, and edited the manuscript.
Funding: Luca Zazzeron was supported from the grant T32GM007592.