Article Type: Case Report, Volume 2 Issue 2
*Corresponding author: Steven Laxton
Emergency Medicine, Ascension St Thomas Hospital, Murfreesboro, USA.
Email: steven.laxton@ascension-external.org
Received: Jun 27, 2025 Accepted: Jul 11, 2025 Published: Jul 18, 2025
Citation: Laxton S, Whetstone D, Wear C. Heterotopic pregnancy in a patient with prior ectopic pregnancy: Case report. Ann Case Rep Med Images. 2025; 2(2): 1028.
Copyright: Laxton S et al. © All rights are reserved
This report is of a case of a 24-year-old female that experienced a heterotopic pregnancy with rupture of the ectopic with a history of an ectopic pregnancy that occurred 2 years prior. This report serves to add to current medical literature a case of heterotopic pregnancy which is alone a rare occurrence and occurs almost exclusively in medically induced pregnancies (i.e. in-vitro fertilization). In this case, a heterotopic pregnancy occurring in a non-medically induced birth is all the rarer. An additional aspect that makes this case report unique is the occurrence in a patient with a prior ectopic pregnancy and secondary to the prior ectopic had a unilateral salpingectomy suggesting that the heterotopic pregnancy resulted from a single ovary.
Heterotopic pregnancy is an exceedingly infrequent phenomenon that occurs when a patient who is pregnant has a concomitant intrauterine pregnancy as well as an ectopic pregnancy, deeming it a heterotopic pregnancy. A prior study to investigate the incidence showed it to be around 0.2% among patients receiving in vitro fertilization therapy [1] suggesting it should be a much lower incidence among non-medically induced pregnancies and from review of literature the occurrence in non-medically induced pregnancies is so infrequent that there is not currently enough data to calculate the incidence. The patient described in this report also had a prior pregnancy that resulted to be ectopic with rupture requiring surgical removal and unilateral salpingectomy. Ectopic pregnancy also occurs infrequently with an estimated incidence, among a few studies, ranging from 6.4 to 20 per 1000 pregnancies [2-4]. The patient in this report presented with RLQ pain for three days and had a negative home pregnancy test but was found in the emergency department to have a positive pregnancy test and then discovered on ultrasound to have an intrauterine pregnancy and right sided ectopic pregnancy with free fluid in the pelvis to suggest rupture of the ectopic pregnancy, i.e. a heterotopic pregnancy with rupture.
The patient was a 24-year-old G3P0030 with a history of prior miscarriage and prior ectopic pregnancy requiring surgical removal and right sided tubal ligation. This patient presented to the emergency department with complaints of abdominal pain and vaginal bleeding for one day. The patient reported abdominal pain in the lower right quadrant that was associated with non-bloody, nonbilious emesis. The patient reported no current medical conditions but did report a history of a prior ectopic pregnancy that required left sided salpingectomy approximately three years prior. The patient reported that approximately six weeks prior to presentation she had a positive home pregnancy test but on the day of presentation she repeated it and resulted negative thus casting doubt that the current pathology was of obstetric origin.
The physical examination was noted to have unremarkable vital signs with temperature of 98.6 F, heart rate of 89, respiratory rate of 18, and a blood pressure of 104/68. The physical examination was most notable for abdominal tenderness in the right lower quadrant with guarding and no rebound. The remainder of the physical examination was unremarkable and without pertinent findings.
Labs were reported to show a positive qualitative pregnancy test which was later repeated for a quantitative serum HCG which resulted at 21218 IU/L, a Complete Blood Count (CBC) without anemia, and a Complete Metabolic Profile (CMP) that was remarkable for a mild elevation in total bilirubin of 2.2 mg/ dL and non-elevated direct bilirubin of 0.6 mg/dL which is nonspecific.
With the initial report of a negative home pregnancy test, a CT scan was ordered for concern of appendicitis as the reported “negative” home pregnancy test made the diagnostic process focus less on pathology of obstetric origin. However, upon receiving the result of bedside pregnancy test being positive in the emergency department the initial workup was then transitioned to a transvaginal ultrasound as the concern for obstetric pathology rose to the top of the differential diagnosis. The ultrasound revealed an intrauterine pregnancy without fetal heart tones suggesting fetal demise as well as a right sided pelvic mass with free fluid seen in the pelvis concerning for ectopic pregnancy was reported raising the concern for heterotopic pregnancy with rupture of the ectopic pregnancy. The on-call obstetrician was immediately contacted, and the patient was taken promptly to surgery for right salpingectomy and dilation and curettage for missed abortion.
In surgery, the uterus was visualized laparoscopically with appropriate size and no obvious abnormalities, the left fallopian tube was visualized as surgically absent from prior ectopic pregnancy consistent with patient’ history. The right fallopian tube, however, was visualized as significantly abnormal with concern for ectopic pregnancy. There was also noted extravasation of blood from the right fallopian tube and pooling of blood in the pelvis confirming the preoperative concern for ectopic pregnancy.
The right fallopian tube was sent for pathology review which showed immature chorionic villi consistent with ectopic pregnancy.
The patient then had an uneventful recovery and was discharged home without complication.
The patient followed up in clinic two weeks following the procedure and was without complications noted and routine follow-up was then established.
Heterotopic pregnancy is a pregnancy that is exceedingly rare among young and healthy women. This condition is usually exclusively related to medically induced pregnancies (in vitro fertilization, super ovulation, etc.) It is not well studied among non-medically induced pregnancies due to how exceedingly rare this condition is.
As previously discussed, heterotopic pregnancy (Figure 1) is an exceedingly rare phenomenon that occurs when a patient who is pregnant has an intrauterine pregnancy as well as an extrauterine (ectopic) pregnancy. In prior studies the incidence was shown to be around 0.2% among patients receiving in vitro fertilization therapy suggesting it should be incredibly lower incidence among non-medically induced pregnancies. The patient in this report also had a prior pregnancy that was ectopic and ruptured which is also a rare occurrence with an estimated incidence among a few reports to estimate an incidence of 6.4 to 20 per 1000 pregnancies [5].
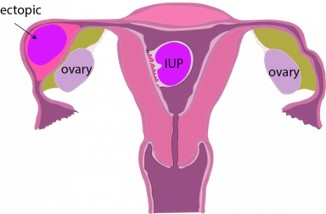
Figure 1:
Heterotopic pregnancy occurs when a blastocyst becomes implanted in both intrauterine and extrauterine locations. Most commonly the ectopic implantation occurs in the fallopian tube at the ampulla (Figure 2) however it can implant in many other sites including ovarian, intestinal, etc.
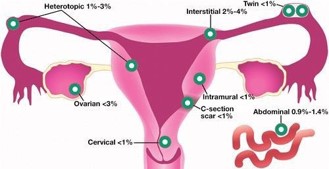
Figure 2:
Most commonly a patient that is experiencing ectopic or heterotopic pregnancy will present with vaginal bleeding and abdominal pain in the first trimester [5]. However, they can also be asymptomatic and present in a myriad of different ways such as back pain, rectal bleeding, syncope, etc. therefore clinicians should always maintain ectopic on the differential diagnosis in a patient of reproductive age. In most instances, heterotopic/ectopic pregnancy falls off the differential diagnosis once a transvaginal ultrasound reveals an IUP especially due to the exceeding rareness of a heterotopic pregnancy. In patients who have undergone pregnancy with assisted reproduction technology, heterotopic pregnancy should remain on the differential diagnosis despite a confirmed intrauterine pregnancy. When evaluating a patient with concern for heterotopic pregnancy there should be special care taken to not only examine the uterus but also the adnexa, assess for free fluid (Figure 3), and special care to look at the fallopian tubes.

Figure 3:
The patient in this report presented with right lower quadrant pain for three days and had a negative home pregnancy test. This as one can imagine from the diagnostic perspective would change the workup and management as well as differential diagnosis quite dramatically however fortunately prior to performing a CT scan of the abdomen and pelvis the pregnancy test resulted and was positive which prompted a pelvic ultrasound to be performed. This ultimately led to the diagnosis of heterotopic pregnancy with rupture.
When determining the management for heterotopic pregnancy it should be determined if the intrauterine pregnancy is live. If so, then medical therapy such as methotrexate would be contraindicated, and the desired therapy would be surgical or other specialized care for treatment of the extrauterine pregnancy. The standard surgical approach would be to perform a salpingectomy (if located within the fallopian tubes) of the extrauterine pregnancy especially if ruptured or hemodynamically unstable [6]. An additional therapy that is alternative to medical therapy would be a local feticidal injection by ultrasound guidance where potassium chloride or hyperosmolar glucose are injected into the ectopic pregnancy. This should only be performed in hemodynamically stable and unruptured ectopic pregnancy [7]. However, despite the approach taken to manage heterotopic pregnancy there is still an increased risk of spontaneous abortion of the intrauterine pregnancy [8].
When deciding plan of care if it is determined that the intrauterine pregnancy is not viable in addition to an ectopic that is unruptured in a hemodynamically stable patient then medical therapy is an option that can be considered. The mainstay of pharmacologic treatment is methotrexate. It is important to remember though that special surveillance should be taken in this patient population since hemorrhage [9] from an ectopic pregnancy is still the leading cause of maternal mortality in the first trimester [10]. Thus, if choosing medical therapy, it should be determined that the patient is not hemodynamically unstable, an intrauterine pregnancy is not present, and there are no signs of impending rupture of the extrauterine pregnancy [11].
Another care that should also be taken is that most of the patients experiencing heterotopic pregnancy have struggled with infertility and after experiencing this pathology will suffer from increased infertility due to scarring of the fallopian tube if feticidal injection is performed or salpingectomy which results in complete removal of one fallopian tube thus greatly reducing fertility. This can lead to greater grief in this patient population, especially if the intrauterine pregnancy is lost as well.
In this case, surgical management was chosen for primary therapy due to the extrauterine pregnancy having signs of rupture with free fluid seen in the pelvis and as seen on ultrasound the intrauterine pregnancy was shown to have fetal demise a dilation and curettage was performed for removal.
In conclusion, heterotopic pregnancy, although infrequent, should be on the differential diagnosis of any female of childbearing age when presenting to the emergency department with abdominal pain, vaginal bleeding, or abnormal or unstable vital signs. It should be especially higher on the differential diagnosis if the patient reports recent attempt of pregnancy or current pregnancy though reproductive assistance technology which will increase the risk of experiencing a heterotopic pregnancy. Management can be medical, however most heterotopic pregnancies are managed surgically. If a heterotopic pregnancy is present, regardless of hemodynamic status, an obstetric physician should be consulted for further management.
Informed consent: Written informed consent was obtained from the patient prior to writing and publication of this case report.