Article Type: Research Article, Volume 2 Issue 1
*Corresponding author: Daniel Simões de Oliveira
Alceu de Campos Rodrigues, 126 - Vila Nova Conceição, São Paulo / SP – Brazil.
Email: danieloliveira8@live.com
Received: May 15, 2025 Accepted: Jun 13, 2025 Published: Jun 20, 2025
Citation: Oliveira DS, Setuguti DT, Melo RAB, Siqueira LTB. Unresectable pancreas cancer: Analysis of safety and efficacy of irreversible electroporation in elderly patients. Ann Case Rep Med Images. 2025; 2(1): 1026.
Copyright: Oliveira DS et al. © All rights are reserved
Introduction: The objective of our study is to present our experience in Irreversible Electroporation (IRE) in the treatment of unresectable pancreas cancer in elderly patients.
Materials and methods: A retrospective study with ten patients over 80 years old who underwent percutaneous or surgical IRE to treat unresectable pancreas cancer between 2021 and 2024 after a multidisciplinary tumor board approval. The procedures were performed with the electroporation device NanoKnife (AngioDynamics, Queensbury, NY). Preoperative data collection included patient demographics along with previous oncologic treatments and Computed Tomography (CT) or Magnetic Resonance Image (MRI). Operative and post-operative assessment involved number of probes, number of pulses, initial and final current and immediate and 30-days complications.
Results: All patients in the study successfully underwent the planned treatment. The mean age was 86 (81-92) years old. Six patients (60%) had previously undergone chemotherapy and/or chemoradiation therapy with stable disease in 80% and partial response in 20% before IRE. 10% of the procedures was performed surgically and 90 % percutaneously CT guided. The mean number of probes was 3 with a total voltage range of 2850 V. The mean procedure time of IRE was 18 minutes. Adverse events occurred in two patients (20%), all being grade I-II complications (one in 48 hours and another within 30 days).
Conclusion: Our initial experience shows that IRE is a feasible and safe option for the treatment of locally advanced pancreas cancer in elderly patients. Short term data seems to be promising but longer follow-up is necessary to verify oncological results.
Keywords: Irreversible electroporation; Locally advanced pancreas cancer; Computed tomography; Magnetic resonance.
Locally Advancer Pancreatic Cancer (LAPC) is one of the most aggressive neoplasms, with a one-year survival rate <20% [1]. Surgical resection with adjuvant chemotherapy is considered the best treatment option, however, fewer than 15% of patients present with resectable disease, although it is the best option, many older patients are not recommended for surgery. In addition, they are also less likely to receive chemotherapy compared with younger patients [2,3].
The incidence of pancreatic cancer increases with age. In the United States, only 13% of all patients with pancreatic cancer are diagnosed before 60 years of age. Elderly patients (>65 years) represent a special subgroup because of the presence of related pharmacodynamic and pharmacokinetic changes [4]. Hence, a standard clinical evaluation of these patients may not be sufficient to determine individual treatment strategies, therefore, therapeutic approaches to this subgroup are a daily challenge.
IRE emerges as a promising technology that achieves similar ablative treatment areas with the advantage of not using thermal effects. Instead, it uses high-voltage electrical pulses (up to 3 kV/cm) that open nanopores in the cell membrane’s lipid bilayer, disrupting cellular homeostasis and leading to apoptosis [5-7], keeping the extracellular matrix unimpaired [8]. Due to the non-thermal ablative technology, IRE has the potential to overcome the problem of difficult tumor location faced by the other ablative methods in LAPC.
Due to advances in modern medicine, with early diagnosis and targeted effective treatments, patients currently have a higher life expectancy than in the last century [9]. This impacts on a broad biopsychosocial issue in how we are treating patients of different ages and backgrounds, using the same generalist data from the studies. Elderly patients, and especially those with multiple comorbidities, have important surgical risks [10,11], in addition to suffering much more with chemotherapy regimens [12,13].
The purpose of the present study is to present our experience in irreversible electroporation in the treatment of unresectable pancreas cancer in elderly patients.
Patients
Clinical data from 2021 to 2024 of the first 10 consecutive patients who had undergone percutaneous or surgical IRE therapy were enrolled for the present analysis; there were nine patients treated percutaneously and one patient treated by open surgery (Table 1). All indications were discussed in the Institution’s Tumor Board with a multidisciplinary team (oncologist, interventional radiologist, and surgeon). The study was approved by the Ethics Committee of our hospital and the written informed consent was obtained for the procedure.
Definitions
Technical success was defined as the successful delivery of the planned therapy in the operation room. Procedure-related Adverse Events (AE) was defined as a complication occurring within 30-days of treatment, according to CTCAE version 5.0 (Common Terminology Criteria for Adverse Events).
IRE Procedure
A Contrast-Enhanced Computed Tomography (ceCT) or MRI scan was performed before the procedure to determine the size and shape of the tumor and its proximity to surrounding structures and the required number of electrodes and their insertion position were planned based on this scan. All patients underwent general anesthesia with standard endotracheal intubation and complete muscular relaxation with heart frequency control between 65-85 bpm. For open surgical patients, a superior midline incision was placed, and the pancreas was exposed at the surgeon’s discretion.
The positioning of the monopolar probes was guided exclusively by high-frequency transducer when surgically treated and CT and US-guided when performed percutaneously. The probes were placed precisely parallel with the inter-electrode distance probe within 1.5-2.2 cm and probe exposure varying between 1.5-2.0 cm, depending on the primary treated site. After probe positioning, twenty 1500 V/cm test pulses were delivered to evaluate the electrical current between probes. An initial current of 20-40A was required and manual parameter adjustment or probe replacement was made if excessive or insufficient energy was detected. Once calibrated, one ECG-synchronized cycle of 90 pulses (pulse length of 90 µs; maximum voltage of 3000 V) was performed. If a current change of >20% of the initial current was not achieved, a second cycle of 60 pulses with the same parameters was performed.
Follow-Up
During the hospital stay, patients were closely monitored and ceCT was performed in case of abnormal clinical signs or symptoms. After discharge, patient was remotely assessed for clinical follow-up and after 12 weeks a ceCT or MRI was performed to evaluate late complications.
Patient’s characteristics
Baseline patient and tumor characteristics are provided in Table 1. In total, 10 patients (5 men, 5 women) underwent IRE for LAPC, with a mean age of 86 (81-92) years old. The median time between diagnosis and IRE was 6 months (range 1–9 months). Six patients (60%) had previously undergone multiple rounds of chemotherapy and/or chemoradiation therapy and one (10%) had upfront surgery. In the pancreatic lesions, 60(60%) was located in the pancreas head; 3 (30%) was located in the pancreas body and one (10%) in tail. The median baseline tumor diameter of the longest axis was 1.9 cm (range 1.2 – 2.2 cm).
Technical outcomes
Details of the procedures are summarized in Table 2. Technical success was achieved in all patients. The median number of electrodes used was 3 (range 2-4). The number of cycles per electrode was in the range of 2; inter-electrode distance was in the range of 1.5 cm; voltage was in the range of 2850 V; and the tip exposure length was in the range of 3 cm. Most patients (n=6, 60%) required 1–2 electrode pull-back techniques to treat target lesions >14 mm. The mean current before and after IRE was 32.2A (range 25.4-40.1 A) and 42.0 A (range 31-48 A). The median duration time from the start of the first cycle until the end of the last cycle was 18 minutes (13-22 minutes); percutaneous and surgical approach median time was 18 minutes and 13 minutes, respectively.
Follow-up
The median in-hospital stay after IRE was 3.8 days, 2 days (13) for percutaneous procedure and 7 days for surgery. Table 3 lists procedure-related adverse events, being 2 (20%) grade 1-2. All patients with minor complications recovered completely following conservative management. In all patients treated for LAPC, before IRE, the median serum levels of amylase and lipase were 55 U/L and 27 U/L, respectively. These values increased to 79 U/L (average increase of 43%) and 49 U/L (average increase of 81%), respectively, one day after IRE. However, these values normalized within one week after IRE and no clinical manifestation was noticed.
| Patient | Age | Gender | Location | Previous treatment | Approach | Lesion size (cm) |
|---|---|---|---|---|---|---|
| #1 | 92 | Male | Head | None | Percutaneous | 1.8 |
| #2 | 89 | Female | Tail | None | Percutaneous | 1.7 |
| #3 | 82 | Female | Body | FolfiRINOX | Percutaneous | 1.9 |
| #4 | 81 | Male | Head | FOLFIRINOX | Surgical | 2.2 |
| #5 | 85 | Male | Head | None | Percutaneous | 2.0 |
| # | 82 | Female | Head | FOLFIRINOX | Percutaneous | 2.1 |
| #7 | 85 | Male | Head | FOLFIRINOX | Percutaneous | 1.7 |
| #8 | 90 | Male | Body | None | Percutaneous | 1.6 |
| #9 | 91 | Female | Head | FOLFIRINOX | Percutaneous | 1.9 |
| #10 | 83 | Female | Body | FOLFIRINOX | Percutaneous | 2.1 |
| Total | Percutaneous | Surgery | |
|---|---|---|---|
| Number of patients | 10 | 9 | 1 |
| Male: n (%) | 5 (50%) | 4 (45%) | 1 (100%) |
| Female: n (%) | 5 (50%) | 5 (55%) | 0 |
| Median age: years (IQR) | 86 | 86 (82-92) | 82 |
| Tumor location: n (%) | |||
| Head | 6 (60%) | 5 (55%) | 1 (100%) |
| Body | 3 (30%) | 3 (33%) | 0 |
| Tail | 1 (10%) | 1 (11%) | 0 |
| Median tumor size: cm (IQR) | 1.9 | 1.8 (1.2-2.1) | 2.2 |
| Median number of probes: n (range) | 3.0 | 2 (2-4) | 3 |
| Median inter-electrode distance: cm (range) | 1.5 | 1.6 (1.3-2.0) | 1.4 |
| Median procedure time (minutes) | 18 | 22 | 13 |
| Median hospital stay: days (range) | 3.8 | 2 (1-3) | 7 |
| Adverse event (NCI-CTCAE) | Grade 1-2 | Grade 3 | Grade 4 | Treatment |
|---|---|---|---|---|
| Gastrointestinal | ||||
| Vomiting | 1 | 0 | 0 | Hospitalization with IV hydration and symptomatic medications |
| Abdominal fluid collection | 1 | 0 | 0 | Percutaneous drainage during hospitalization |
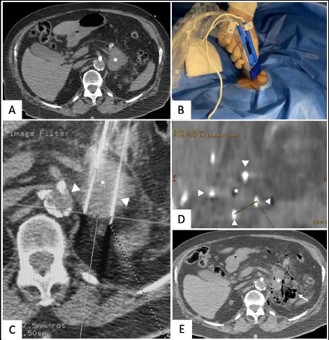
Figure 1: Percutaneous IRE of a local pancreatic recurrence.
(A) Pre-treatment CT showing local recurrence (asterisk);
(B) Percutaneous positioning of the probes;
(C) Probe (arrowhead) positioning confirmation within the tumor (asterisk);
(D) Inter-electrodes measurements (dashed line) between the probes (arrowhead);
(E) Immediate CT after IRE shows the lesion (asterisk) with similar aspect surrounded by gas (arrow).
Demographic aging has been a constant in recent decades worldwide. According to the United Nations, the number of elderly people aged 60 or over is expected to double by 2050 and more than triple by 2100, from 962 million in 2017 to 2.1 billion in 2050 and 3.1 billion in 2100 [14]. The association between aging and cancer is well established: carcinogenesis is a timeconsuming process with a final product (cancer) that is more likely to occur late in life; older tissues are more vulnerable to environmental carcinogens; and changes in the environment of the body (chronic inflammation, immunosenescence) may favor the development of cancer [15,16]. Additionally, the immune system plays an important role in the progression of pancreatic cancer [17-19]. Some studies have shown that nearly half of all elderly patients did not receive any treatment for locoregional pancreatic cancer. Moreover, only 11% received a multimodal therapy (surgery +/chemoradiotherapy) [20].
In elderly patients, the use of chemotherapy is often limited due to the increased risk of adverse events related to comorbidities, poor performance status, or poor cognitive function [21]. Only a few studies have provided information on the tolerability and benefits of chemotherapy in the elderly [22-24]. A previous study showed that many patients receiving chemotherapy for incurable cancers might not understand that chemotherapy is unlikely to be curative [25]. On the other hand, there may be several reasons why elderly patients tend to choose Best Suportive Care (BSC) over chemotherapy, which are likely to include organ dysfunction, drug toxicity, and a refusal to give informed consent. The greater susceptibility of elderly patients to severe drug toxicity that is most likely due to the age-related deterioration of organ function and/or drug clearance, and other disorders that may contraindicate chemotherapy [26].
An important parameter to discuss in detail with elderly patients, who are considered as candidates for surgery, is not only the potential survival benefit but also the postoperative quality of life and functional recovery [27]. 40% of patients between the ages of 66-70 years are candidates for a pancreatectomy, but by the age of 85 years, only 7% are eligible candidates [28,29]. A meta-analysis of nine studies evaluating the outcome of pancreatic resection in octogenerians revealed significantly higher morbidity and mortality in this age group compared to younger patients. The difference however was not significant when comparing patients with similar comorbidities [30]. According to the results in patients >75 years old with locoregional disease, surgery alone or in combination with chemotherapy did not result in improved survival compared with no treatment [31]. Minimally invasive surgery is associated with a lower rate of cardio-respiratory complications, diminished post-operative pain, shorter hospital stays, and a faster reincorporation into daily activities. Therefore, it is a very good option for elderly patients [32].
The development of IRE to treat LAPC, which induces nonthermal tissue necrosis through high-voltage electrical pulses that determine nanopores in cell membrane from tumor cells [33], preserving adjacent tissues such as vessels, nerves, and bile ducts [34] opened a new era in the treatment of patients whose prognosis is more reserved, mainly due to the worse functional reserve due to advanced age. IRE can be performed percutaneously, guided by ultrasound and computed tomography, which implies less metabolic stress for the patient when compared to open surgery. Many studies have investigated the outcomes of percutaneous IRE under CT guidance in patients with LAPC [35-37]. Narayanan et al. [38] reported a median OS of 14.5 months from the date of IRE with no procedure-related deaths for percutaneous IRE, which is similar to those reported for intraoperative IRE [39,40]. In our initial experience, nine patients have successfully undergone percutaneous IRE and one received the surgical approach. The choice for the surgical approach was mainly because all patients had borderline surgical LAPC and IRE was planned to treat only in the region where the surgeon could not withdraw the tumor with safe margins.
Several studies have reported major complications, in the range of 19%-59% [33,41], including hemorrhage from gastrointestinal ulceration, vessel stenosis, or bile duct injury [41,42]. In the present study, there was no death within the one-month follow-up period. One patient in the percutaneous approach presented with persistent vomiting requiring endovenous medication and fluid hydration; another patient presented fluid collection in the abdominal cavity that was percutaneously drained and considered most likely to be related to the surgery. In the present study, patients treated for LAPC had transient elevation of serum amylase and lipase levels one day after IRE, returning to normal values one week after IRE. This result could be due to transient inflammation of the pancreas after inserting the electrode during the procedure [43]. No clinical significative pancreatitis was observed in our patients.
Limitations
The present study has some limitations. First, this study included a small number of patients and the follow-up time after IRE was relatively short. Second, there was no control group, such as patients undergoing conventional chemotherapy, to compare. Further randomized controlled studies are needed to overcome these limitations.
In conclusion, for elderly patients with LAPC, IRE appears to be a promising treatment modality with an acceptable safety profile. However, prospective studies with a control group are necessary to determine the efficacy of IRE.