Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Anas Hamdoun
Department of Medical Imaging, King Abdullah bin Abdulaziz University Hospital, Riyadh, KSA.
Email: aohamdoun@kaauh.edu.sa
Received: May 03, 2025 Accepted: Jun 05, 2025 Published: Jun 12, 2025
Citation: Hamdoun A, Awad MA, Alajlan Z, Khubrani R. Anterior abdominal wall lipoma, mimicking adnexal lesion: A case report. Ann Case Rep Med Images. 2025; 2(1): 1024.
Copyright: Hamdoun A et al. © All rights are reserved
Although lipomas are the commonest abdominal wall masses, the ones related to the peritoneum are extremely rare. We present here the second one in the literature and the first one mimicking ovarian dermoid for a 28-yearold lady who presented with right lower quadrant acute abdominal pain. The laboratory investigations were normal and both ultrasound and MRI were suggesting right ovarian dermoid.
Since she presented with acute abdomen and torsion de-torsion could not be ruled out, she was taken to OR. Operatively, no adnexal mass was seen, however, a right lower pelvic mass arising from the peritoneum related to the anterior abdominal wall just anterior to the right adnexa. The mass was dissected and sent to histopathology which revealed features of lipoma with no malignant changes.
A 28-year-old female, presented to the emergency department with an acute right lower quadrant pain. She has regular periods without intermittent bleeding or heaviness. The laboratory investigations upon presentation were normal. They decided to do a pelvic ultrasound to rule out ovarian torsion. She also reported history of pelvic mass and brought an MRI done previously for the same reason.
The ultrasound (Figure 1) showed a welldefined ovalshaped homogenously echogenic right pelvic mass inseparable from the right ovary without internal-vascularity measuring 5.4 × 3.6 × 3.9 cm with no sonographic evidence of ovarian torsion. Review of the MRI pelvis (Figure 2) revealed right sided pelvic non-enhancing mass which again did not appear separable from the right ovary, therefore reported as right adnexal/ovarian dermoid. The mass is also noted to be abutting the lower right anterior abdominopelvic wall, which could be a usual appearance for any sizable ovarian mass.
She was then taken to the OR. Intraoperatively, using laparoscopic approach, the uterus, ovaries and tubes are noted to be healthy bilaterally with no adnexal mass. However, a yellowish sessile anterior abdominal wall mass was noted on the right side attached to the peritoneum and protruding into the right hemipelvis with minimal omentum adherent to it (Figure 3) which was easily dissected and the mass was removed in toto.
The histopathology revealed benign fibrofatty tissue with fat necrosis, acute inflammation and granulation tissue. Negative for malignancy (Figure 4).
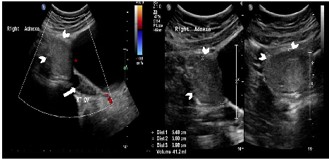
Figure 1: Pelvic ultrasound showing the right ovary (white arrow) and the echogenic right pelvic mass apparently inseparable from it (white arrow heads).
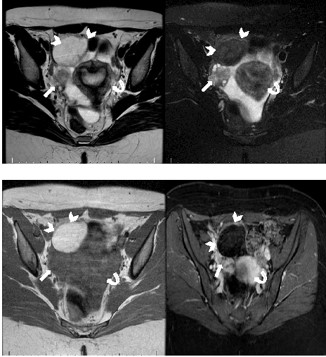
Figure 2: Pelvic MRI (A) Axial T2 (B) Axial T2 with fat saturation. (C) Axial T1 without fat saturation and (D) Axial T1 with fat Saturation Post contrast showing: the right ovary (white arrow), the mass (white arrow heads) and the uterus (white curved arrow).
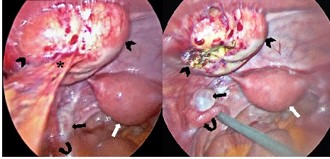
Figure 3: Laparoscopic operative photos: (A) before being freed from omental adhesions (asterisk) and (B) after: showing the anterior abdominal mass (arrow heads), the right ovary (black arrow), the right fallopian tube (curved arrow) and the uterus (white arrow).
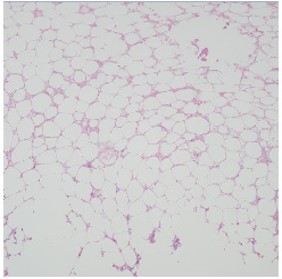
Figure 4: Histopathology result revealed: A typical fibrofatty lesion in keeping with lipoma with no features of malignant transformation.
Pelvic pain in women of child bearing age is quite common in emergency departments. Ovarian etiology of such pain is also the commonest amongst others. In such patients, appropriate history taking and clinical examination in addition to laboratory investigations will point out diagnosis. Bedside ultrasound has a great role in diagnosis and further cross-sectional imaging, with CT or MRI is usually spared as trouble shooting or problemsolving techniques, particularly, if alternative diagnosis is to be considered.
Lipomas are slow growing benign fatty tumors, accounting for about 50% of the soft tissue tumors [2]. They are the most common abdominal wall and subcutaneous tumors [2,7,10]. The peak of the affected age is between the 40-70 [7,9]. Those lesions can be seen in singular or multiple pattern, in the deep or superficial structures [7]. These tumors are composed of differentiated adipose tissue with adjacent fibrous capsule. The classical pattern of lipomas are found to be incidental finding in most of the cases. Tumor size, shape and relation to surroundings are significant to cause symptoms [9].
Benign pelvic lipomas are the most common mesenchymal lesions which can be seen anywhere in the human body [4,7,9,10]. The tumors that contains fat are seen within the female pelvis are common findings. The majority of these lesions are benign in nature such as cystic ovarian teratoma or lipomatous lesions of the uterus [4]. Ovarian teratomas are the most common germ cell neoplasms. By far, most ovarian teratomas are mature cystic teratomas, also known as dermoid cysts [13]. Most of these tumors are treated surgically, however, in asymptomatic patient it doesn’t need any treatment, particularly if they are small in size.
Although lipomas are the commonest abdominal wall masses, the ones related to the peritoneum are extremely rare [7,14,15]. We are reporting the first case, to the best of our knowledge presenting with one mimicking ovarian teratomas with no features of torsion or degeneration. However, it is noted to have some omental adhesions which are thought to be the possible cause of the on and off pain.
The diagnostic approach for patients presenting with pelvic pain is well established. The workup for adnexal masses as a cause is also well described in the literature, emphasizing the role of medical imaging. The fat content in masses along with their relations to surroundings using cross-sectional imaging is also well featured.
The role of ultrasound in diagnosing or confirming fat containing masses, like lipomas and teratomas is well established [10]. However, the appearance of such masses in the ultrasound have been variable with the echogenicity of the lesion may be ranging from hypoechoic to isoechoic depending into the connective tissue within the lesion [10]. On the other hand, superficial lesions can be assessed utilizing ultrasound as in the anterior abdominal wall lesions [2] since it`s a dynamic procedure.
Usually, clinical assessment and ultrasound will solve most of the clinical dilemmas. However, further cross-sectional imaging with CT or MRI might be indicated in some scenarios, as trouble shouting modalities, depending on the clinical scenarios. Magnetic resonance imaging is nonradioactive tool which dispenses high-resolution images with best characterization of soft tissues, particularly for fat. MRI is crucial in pre-operative planning, as it provides an accurate location, mass size, and the relation of the adjacent structures to the lesion itself [2]. The appearance of lipomas in MRI are homogeneous well-defined manure adipose tissue signals: T1 and T2 sequences high signal intensity, possible thin fibrous capsules are seen within the lesion [2]. T2-weighted images with fat suppression will show low signal intensity of the lesion with high signal intensity of the internal fibrous capsule [2]. IV Gadolinium contrast injection is used to show possible features of malignant transformation, if suspected.
Computed tomography is excellent for characterizing the fatty tissues in tumors using the Hounsfield units (HU) which accurately characterize the fat density in lesions. On CT, areas of low attenuation (<-20 HU) have been accepted as evidence of fat within tissues and classic lipomas generally have HU measurements between (-65 and -120) with fat within the lesions resembling subcutaneous fat [11]. At CT, fat attenuation within a cystic adnexal mass, with or without calcification in the wall, is diagnostic of ovarian teratomas [13]. However, because of its inherent radiation dose, MRI is preferred in most of the cases. On the other hand, despite the known role medical imaging in lipomas in general, most of the intra-abdominal ones are found at times of surgery [7]. Therefore, higher rate of suspicion is suggested in image interpretation with more application of dynamic and case-based techniques to avoid guide appropriate decision making and avoid unnecessary interventions.
Anterior abdominal wall lipomas related to the peritoneum are extremely rare which may rarely be confused with common pelvic pathology. A high index of suspicion is required to prompt adequate cross-sectional imaging and accurate diagnosis to consequently guarantee appropriate management and surgical intervention, when indicated.