Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Biswajit Mishra
Department of Plastic Surgery, SCB Medical College, Cuttack, Odisha, India.
Email: drbmpl78@gmail.com
Received: April 22, 2025 Accepted: May 06, 2025 Published: May 13, 2025
Citation: Mishra B, Roy S, Nayak BB, Parashar M, Sahoo V. Pseudoaneurysm: A case report. Ann Case Rep Med Images. 2025; 2(1): 1022.
Copyright: Mishra B © All rights are reserved
Pseudoaneurysms of the superficial palmar arch are rare entities and only a few cases have been described in the English literature [1-10]. Penetrating trauma, repetitive trauma to a particular point is common aetiology. They can occur as a complication after previous surgery like carpal tunnel release [1] and arterial puncture. Most of the cases have been reported in paediatric age group [2-4,7,8] very few cases are reported in elderly [9].
We present a case of 80-year-old female presented to plastic surgery OPD with chief complaint of swelling in right hand for last 1.5 months.
She was operated for trigger finger of right hand at a private nursing home. 15 days later, she developed a swelling over the operated site which gradually increased in size to size of 2 cm × 1.5 cm. The swelling was associated with mild pain.
On local examination, the swelling was situated over palmar aspect of right hand, soft in consistency, immobile, globular in shape, margins well defined, expansile in nature, with local rise in temperature, mild tenderness on touch. There was discoloration of the skin overlying the swelling. There was no functional or sensory impairment.
USG Finding revealed a well-defined hypoechoic region showing normal vascular flow with possible communication to interdigital artery noted in subcutaneous layer of right palm most likely pseudoaneurysm (Figure 1).
Figure 1: USG Report.
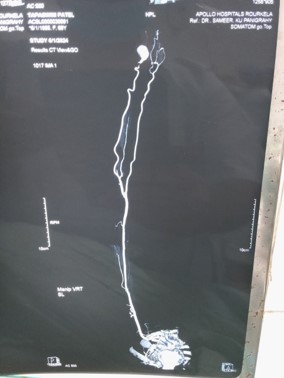
Figure 2: CT angio report.
CT angiography – revealed well defined ovoid outpouching fed by ulnar artery measuring 21 mm x 18 mm in cross section suggestive of pseudoaneurysm of superficial palmar arch (Figure 2).
Patient was operated under brachial block anaesthesia. Tourniquet was applied. Longitudinal incision was given over swelling (Figure 3). Subcutaneous tissue dissected and Capsule of the pseudoaneurysm identified (Figure 4). Digital vessel found to be adherent to the capsule. Digital vessel dissected from the capsule and safeguarded. The base of the pseudoaneurysm was found having communication with the superficial palmar arch (Figure 5). The capsule was opened and the hematoma was evacuated. The communicating vessel with the superficial palmar arch was ligated and the capsule was excised (Figure 6). Hemostasis achieved. Skin closed. Post–op course uneventful (Figure 7). There was no collection, no sensory impairment, no functional impairment.

Figure 3: Intra op.

Figure 4: Clinical image.

Figure 5: Clinical image.

Figure 6: Clinical image.

Figure 7: Clinical image.
Pseudoaneurysms differ from true aneurysms with respect to the distortion of arterial architecture. True aneurysms involve a dilatation of all three layers of the arterial wall without a breach in continuity of the vessel wall while in false aneurysm there is breach in continuity and architectural distortion of the vessel wall. There is a disruption of the vessel wall of the artery and a leakage of arterial blood from the artery into the surrounding tissue with a communication between the originating artery and the resultant adjacent cavity. Hematoma formed initially is covered by a fibrous covering.
They usually present as pain, swelling and a pulsatile mass in the palm near the site of the injury [3,4]. They can present as massive haemorrhage [5] or as carpal tunnel compression syndrome [6]. Most of the cases are reported in paediatric age group [2-4,7,8] Cases have been reported as early as 6-monthold child [2]. Very few cases are reported in adults and elderly age group [9].
An X-ray of the hand can be performed to exclude the presence of a foreign body.
Ultrasound, CT angiography, MR angiography and Stereoscopic MRA are modalities available for diagnosis of the disease. Ultrasonography is the initial diagnosis in the majority of cases. CT angiography can be useful as it can specify the exact location of the aneurysm, the presence of collaterals and may be useful in planning reconstructive surgery, but its use remains controversial due to its potential complications, such as the possibility of distal embolization [1]. Angiography can differentiate the true from the false aneurysms according to their angiographic characteristics: saccular appearance for the false aneurysms and fusiform shape for the true ones [7].
Magnetic Resonance Angiography (MRA) is as useful without necessitating any contrast medium. Also, stereoscopic MRA may provide additional information regarding the location of the aneurysm [8]. Our case has occurred after trigger finger release in an 80-year-old woman. There is no case presented till date due to trigger finger as aetiology.
Treatment can be conservative or surgical. Small, uncomplicated pseudoaneurysms can be managed conservatively by application of compression bandage [4]. However, there is risk of distal embolization with subsequent occlusion of the run-off arteries. Surgical methods include open surgical resection with ligation or arterial reconstruction by end-to-end anastomosis using microvascular technique [7-9]. Recently, endovascular techniques such as coil embolization have been employed with success in the treatment of the false aneurysms of the superficial palmar arch. This minimally invasive method may be an alternative to open surgery in the management of these lesions [1].
Ultrasound-guided thrombin injection has been found to be an effective, time-saving, and safe procedure for treatment of pseudoaneurysms [10], but it should be avoided as treatment for cases with arteriovenous fistula or when the pseudoaneurysm neck cannot be seen Our case has presented at age of 80 years.
Our case has occurred after trigger finger release in an 80-year-old woman. There is no case presented till date due to trigger as aetiology.
In spite of their rarity, pseudoaneurysms of the palmar arch can cause severe discomfort and complications to patients after penetrating injury to the palm of the hand. Accurate diagnosis is based on the awareness of the disease and correct imaging procedures. For that reason, follow-up seems to be necessary after penetrating hand injury in order to diagnose and treat this rare entity. We do not favour conservative treatment as it is associated with high risk of distal embolization but suggest surgical resection with ligation or arterial reconstruction as the treatment of choice.