Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Ilham Snoussi
Department of Dermatology and Venereology, Mohammed VI University Hospital, La Nouvelle Ville Ibn Batouta, Tangier, Morocco.
Email: ilham.snoussi@usmba.ac.m
Received: April 12, 2025 Accepted: May 02, 2025 Published: May 09, 2025
Citation: Snoussi I, Jouari OE, Abbad F, Gallouj S. Abdominal cystic lymphangioma: A rare case of cutaneous congenital malformation. Ann Case Rep Med Images. 2025; 2(1): 1020.
Copyright: Snoussi I et al. © All rights are reserved
Introduction: A uncommon benign lymphatic malformation called Lymphphangioma Circumscriptum (LC) is caused by dilated lymphatic veins in the epidermis and subcutaneous tissue. It frequently manifests in early childhood and can be acquired or congenital. Histopathology, dermoscopy, and clinical characteristics are used to make the diagnosis. Treatment is still difficult because traditional methods such as sclerotherapy and surgery are not very effective. Targeted therapy has been made possible by recent findings of PIK3CA mutations and activation of the PIK3CA/AKT/mTOR pathway; sirolimus (rapamycin) has emerged as a potential alternative despite not having FDA approval.
Case report: We report a 1-year-old boy who has a congenital lesion on his right flank that is getting bigger with time. An erythematous-violaceous plaque measuring 7 cm was found by dermatological examination, with hemorrhagic vesicles that resembled “frog spawn.” Imaging revealed a cystic lymphangioma inside the abdomen. A microcystic lymphangioma was verified by histopathology. Oral sirolimus (0.8 mg/m²/dose, twice daily) was administered to the patient in order to evaluate its efficacy in decreasing the size of the lesion and enhancing the appearance of the skin.
Discussion: According to the ISSVA classification, LC can be categorized as mixed, macrocystic, or microcystic. Dermoscopy, which displays lacunar patterns with bloodfilled spaces, aids in the diagnosis. Histologically, erythrocyte extravasation and lymphatic vessel dilatation are features of microcystic lesions. For microcystic forms, standard therapies including surgery, lasers, and sclerotherapy frequently don’t work. Sirolimus, an antiangiogenic mTOR inhibitor, has had encouraging outcomes in lowering lymphatic abnormalities. Although new data points to its promise for treating LC, more research is required to ensure long-term safety and efficacy.
Keywords: Lymphangioma circumscriptum; Microcystic lymphangiom; Histopathology; Dermoscopy; Sirolimus (rapamycin).
Lymphangioma Circumscriptum (LC) is an uncommon benign lymphatic malformation occurring from lymphatic channel dilation in the epidermis and subcutaneous tissues, often identified in early childhood. It may be acquired after lymphatic injury from illnesses like tuberculosis or filariasis, or it may be congenital or the result of developmental abnormalities. Clinically, LC manifests as translucent vesicles that resemble “frog eggs,” and the gold standard for diagnosis is histology [1]. Microcystic Lymphatic Malformations (MLM) are difficult to treat since they don’t respond well to traditional treatments like sclerotherapy, which has safety concerns [1,2]. Targeted medicines have been made possible by recent findings of PIK3CA mutations and activation of the PIK3CA/AKT/mTOR pathway; sirolimus has emerged as a viable therapy option, albeit one that has not yet received FDA approval [2].
We report on the case of a 1-year-old boy, the family’s second child, who was brought in for treatment of a congenital cutaneous lesion on his right flank. The baby, who weighed 3 kg at birth, was delivered via cesarean section at full term following a well-managed pregnancy. With the recent start of supplemental feeding, he is currently just breastfed. The infant has received all recommended immunizations and is developing psychomotorly normally.
The patient had surgery for a right inguinal hernia when he was six months old. A purple-colored plaque that was somewhat itchy but not unpleasant first appeared on his right flank after birth, marking the beginning of his current skin problem. The parents sought advice from a pediatric facility as a result. A cystic lymphangioma of the abdominal wall was suspected based on an ultrasonography. The parents sought additional medical attention after the lesion clinically became larger and began to release a fluid that resembled blood. The lesion did not improve, therefore a TAP scan was sought and a referral for a potential ultrasound-guided Fine-Needle Aspiration (FNA) was made. An intra-abdominal fluid collection with a thinwalled partition was seen on the CT scan, which may indicate an intra-peritoneal cystic lymphangioma.
The patients phototype upon dermatological evaluation was [3]. A well-defined, irregularly bordered erythematousviolaceous plaque, about 7 cm in diameter, was found on the right iliac fossa during the skin examination. The plaque showed several different-sized vesicles that looked like “frog spawn” because they contained hemorrhagic material (Figures 1,2).
Dermoscopy showed several witish, well-defined, roundish patches (lacunae). Blood was found in only few lacunae, and it was typically gathered in the Dotted vessels and the lowest portion of the lacuna (Figure 3).
A 4 mm punch was used to perform a skin biopsy, and the sample was transported to the pathology lab. A lymphatic malformation and blood extravasation into the cutaneous tissue were confirmed by the histological analysis, which showed dilated lymphatic channels and erythrocytes (Figure 4), confirms the diagnosis of a confined microcystic lymphangioma. To assess the effectiveness of oral rapamycin (mTOR inhibitor) in treating superficial cutaneous involvement of Lymphangioma Circumscriptum (LC), 0.8 mg/m² is given twice daily at 12-hour intervals. The main goal is to evaluate the clinical response, which includes symptom relief, skin appearance improvement, and lesion size reduction. The case follow-up will also concentrate on tracking the development of superficial lesions over time, assessing alterations in lymphatic outflow, vascular anatomy, and possible regression. Understanding the therapeutic role of mTOR inhibition in microcystic lymphatic malformations—an area with few available treatments—may be aided by this case.
Definition
Developmental abnormalities of the lymphatic system that are usually localized are called cutaneous lymphangiomas or Localized Cutaneous cystic Lymphatic Malformations (LCML). There are three types of LCML: mixed, macrocystic, and microcystic [3]. Although these deformities are typically isolated, they can also coexist with more complex deformities [3,4]. Rarely, they appear in maturity, although they usually appear at birth or in early infancy [3,4]. When a persistent swelling or infiltrating plaque is seen on otherwise normal-looking skin, occasionally with vesicles or a few vesicles, the diagnosis is frequently made clinically. Compressive sensations, intralesional hemorrhage, and inflammatory flare-ups are the main side effects of LCML [4].
Classification
Lymphatic malformations are divided into basic and complex varieties according to the 2014 ISSVA (International Society for the Study of Vascular Anomalies) classification [5]. While complex malformations can manifest in conjunction with capillary, venous, and arteriovenous malformations, simple malformations include macrocystic, microcystic, and mixed cystic lymphatic malformations. Gorham-Stout disease, primary lymphedema, and other widespread lymphatic abnormalities are particular instances [5]. These various forms can be combined in diverse patterns to generate complex deformities [6,7].
Cystic lymphangioma
Clusters of translucent vesicles filled with lymphatic fluid are the characteristic hallmark of Cutaneous Lymphangioma Circumscriptum (CLC), which can occur at any age but is most frequently seen in children [8]. Atypical appearances or isolated lesions are also possible. Hemangiomas, angiokeratomas, pyogenic granulomas, angiosarcomas, cutaneous metastases, warts, and molluscum contagiosum are among the differential diagnosis for circumscribed lymphangioma [8].
Dermoscopy
Dermoscopy identifies two main patterns and is essential in the diagnosis of LC. The lacunar pattern exhibits irregular gaps, and the hue of the lacunae varies according on their contents [9]. Normally, lymphatic fluid is light yellow or light brown, but when red blood cells are present in the dilated lymphatic channels, the fluid appears pink or crimson [10]. The term “dark lacunae” refers to thrombosed lacunae that have a dark purple, dark blue, or black appearance. Sometimes there is also a gradient color change from dark at the bottom to light at the top, or a bicolored lacuna. In addition to small linear arteries, which are typical of confined lymphangiomas, the vascular pattern frequently includes red spots or loops encircled by a white halo [10].
Histological appearance
Classifying lesions according to the size of the cystic spaces simplifies the histological categorization of LCML. Microcystic lymphangiomas, also known as capillary or circumscriptum lymphangiomas, are lymphangiomas with chambers smaller than 5 mm [11]. These lesions show dilated lymphatic or epidermal vessels on histology. Given that the location and kind of lymphangioma impact the prognosis and treatment strategy, this classification is important from a clinical and therapeutic standpoint [12].
Ass exploration
Mixed forms of LC can be seen using imaging methods such Computed Tomography (CT) and ultrasonography [13]. Prior to any treatment intervention, Magnetic Resonance Imaging (MRI) is the recommended evaluation since it is the most accurate way to assess the degree of the lesions [13].
Differential diagnosis
The differential diagnosis for circumscribed lymphangiomas includes hemangiomas, angiokeratomas, pyogenic granulomas, angiosarcomas, cutaneous metastases, warts, and molluscum contagiosum. Careful clinical and dermoscopic evaluation is essential for accurate diagnosis [14].
Associations
Frequently occurring within the same lesion, Microcystic Lymphatic Malformations (MLM) can occasionally coexist with other vascular abnormalities. A capillary angioma may occasionally accompany MLM, which would further muddle the clinical picture. Furthermore, MLM may be linked to hereditary disorders including Proteus syndrome, which is characterized by segmental hemihypertrophy, macrodactyly, connective tissue and/or epidermal hamartomas, and flat angiomas [15].
Evolution
The natural progression of LC typically involves relative stability, though flare-ups may occur due to inflammatory episodes [15,16]. These flare-ups are often triggered by infections or trauma and may be accompanied by intralesional bleeding. The swelling, which was previously asymptomatic, can increase in size, becoming erythematous and painful. The impact of these inflammatory episodes depends on the type and location of the LC. Although spontaneous regression is rare, it can occur following an infectious episode that induces inflammatory and fibrotic changes [16].
The management of Lymphatic Malformations (LM) often requires a multidisciplinary approach and an individualized treatment plan based on symptoms, functional impairment, lesion size, and location. Surgery remains a cornerstone of treatment, particularly for microcystic and mixed LM. Sclerotherapy is highly effective for macrocystic LM and is frequently used as an adjunctive therapy in combination with surgery. Various sclerosing agents are available, with picibanil (OK-432) and doxycycline being the most commonly utilized [17,18]. Laser therapy, which facilitates tissue vaporization and the sealing of superficial lymphatic channels, is primarily effective for mucosal LM [19]. In cases where functional deficits and symptoms are absent, a watch-and-wait strategy may also be a viable option. Pharmacological treatment has been explored for large LM, especially in patients refractory to conventional therapies. Among systemic treatment options, sirolimus appears to be the most promising, as it has demonstrated efficacy in inhibiting lymphangiogenesis in certain conditions [19,20]. Sirolimus, also known as rapamycin, was initially discovered in a soil sample from Rapa Nui (Easter Island). It is a naturally occurring macrolide derived from the bacterium Streptomyces hygroscopicus. Sirolimus acts as a specific inhibitor of the mammalian Target of Rapamycin (mTOR), a serine/threonine kinase that plays a crucial role in regulating angiogenesis, cell growth, and proliferation [21]. Approved by the FDA in 1999 as an oral immunosuppressant for renal transplantation, sirolimus was further authorized in 2015 as the first drug for the treatment of lymphangioleiomyomatosis, a rare disease characterized by progressive cystic lung disease, angiomyolipomas, and lymphangioleiomyomas, predominantly affecting young women. Due to its antiangiogenic and antiproliferative properties, sirolimus has been utilized in the treatment of large LM. A previous systematic review demonstrated that sirolimus therapy has the potential to improve symptoms and reduce LM size across various anatomical regions [22].
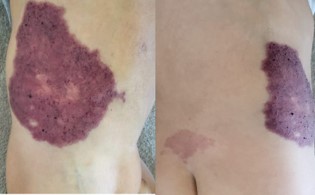
Figure 1 & 2: Reveal a well-demarcated erythematous-violaceous plaque with irregular borders, measuring approximately 7 cm in diameter, located on the right iliac fossa. Several vesicles of varying sizes were noted on the plaque, containing hemorrhagic material, giving them a “frog spawn” appearance.

Figure 3: Dermoscopy revealed multiple witish well-circumscribed roundish areas (lacunae). Few lacunae contained blood, which was characteristically accumulated in the lowest part of the lacuna and dotted vessels.
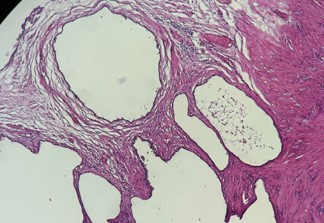
Figure 4: Histological image (case report discussed – hematoxylineosin staining, x20) showing a lymphatic proliferation. It forms variably sized, cystic-like slits. The lumen contains fibrinous sheets.
Lymphatic Malformations (LM) are congenital anomalies of the lymphatic system, classified as macrocystic, microcystic, mixed, or superficial circumscribed. The superficial circumscribed form presents as a localized, well-defined lesion, often affecting the skin or mucosa without deep tissue involvement. Treatment depends on size, location, and symptoms, with laser therapy being particularly effective for superficial circumscribed LM. In refractory cases, sirolimus, an mTOR inhibitor with antiangiogenic properties, has shown promise in reducing lesion size and improving symptoms.
Conflicts of interest: There are no conflicts of interest.