Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Nika Samadzadeh Tabrizi
Department of Cardiac Surgery, Cleveland Clinic Foundation, 9500 Euclid Ave, Cleveland, OH 44195, USA.
Email: Nikasamadzn@gmail.com
Received: Feb 04, 2025 Accepted: Mar 18, 2025 Published: Mar 25, 2025
Citation: Addepalli S, Tabrizi NS, Fabian T, Langford S. CMRI in a patient with left-sided cardiac defibrillator: Reducing artifact with fast gradient echo sequencing. Ann Case Rep Med Images. 2025; 2(1): 1017
Copyright: Tabrizi NS et al. © All rights are reserved
Myocardial viability is primarily evaluated with Cardiac Magnetic Resonance Imaging (cMRI); however, patient Implantable Cardioverter-Defibrillators (ICDs) have been shown to increase image artefact and reduce diagnostic viability. A 65-year-old man with ischemic cardiomyopathy, coronary artery disease and an ICD presented with a chief complaint of chest pain and dyspnea. He was first evaluated via Transthoracic Echocardiography (TTE) with an EF of 35-39% which deteriorated to below 25%. Left heart catheterization showed near-total obstruction of the left anterior descending artery. cMRI was then performed using Steady-State Free Precession (SSFP) and fast Gradient Echo (GRE) sequencing with minimum artefact. GRE improved image quality, revealing global hypokinesis and transmural delayed enhancement, suggesting non-viable myocardium. Although, cMRI remains the gold standard for assessing myocardial viability, artifacts from ICDs limit diagnostic utility. GRE sequencing offers a promising alternative by reducing artifacts, particularly in left-sided ICDs.
Learning objectives: Fast Gradient Echo (GRE) sequences can serve as a proxy for the current SSFP sequencing method in cardiac magnetic resonance imaging (cMRI). This is particularly helpful in the case of susceptibility artefact reduction in patients with Implantable Cardioverter Defibrillators (ICDs). Using this method could be used to increase image diagnostic quality and ultimately aid clinical decision-making in patients under examination for myocardial viability.
Keywords: Cardiac Magnetic Resonance Imaging (cMRI); Implantable Cardioverter-Defibrillator (ICD); Device-related artifacts; Fast gradient echo (GRE); Steady-state free precession (SSFP).
Cardiac Magnetic Resonance Imaging (cMRI) is the gold standard tool for evaluating myocardial structure and function. Despite advancements in MRI safety with MR-conditional implantable devices, concerns persist, particularly regarding the interference caused by ICDs. These devices often introduce banding and flow artifacts, leading to non-diagnostic images in nearly a third of patients, especially in patients with left-sided (versus right-sided) ICDs [1,2]. Cine imaging commonly used to measure systolic function, ventricular mass, and chamber volumes is routinely performed utilizing the SSFP sequence [2,3]. This sequence is most frequently affected by device-related artifacts, resulting in a greater number of non-diagnostic images involving the left ventricle compared to the right (47% versus 31%) particularly in the anterior, septal, lateral, and apical segments [1-3]. The generated artifact has the potential to obscure the myocardial segments completely, thereby hindering the assessment of crucial diagnostic factors such as wall motion abnormality and ejection fraction. This is especially critical in patients such as the present case, who are undergoing assessment for surgical candidacy.
A 65-year-old man with multi-vessel coronary artery disease, multiple PCIs, ischemic cardiomyopathy, and a left-sided dual-lead ICD presented with chest pain, dyspnea and pedal edema. His anti-anginal medication was augmented, and TTE was performed with an ejection fraction of 35-39%. A follow-up TTE yielded an ejection fraction of 25%. Left heart catheterization revealed near complete obstruction of the left anterior descending artery.
Cardiac cMRI at 1.5T (GE HealthCare, USA) was used to check for myocardial viability and guide treatment. Imaging was initially conducted with Steady-State Free Precession (SSFP) sequencing, revealing susceptibility artifact related to the ICD (Figure 1A-D).
To reduce the device-related susceptibility artifact, cine imaging was subsequently performed utilizing fast Gradient Echo (GRE) sequencing, revealing global hypokinesis with marked dyskinesis at the apex and the mid-apical septum, myocardial thinning of the lateral, inferolateral, and apical segments, and a severe left ventricular systolic dysfunction with an ejection fraction 28% (Figure 1E & F).
Late gadolinium enhancement was also limited due to susceptibility artifact, especially at the apical, lateral, and basal anterior segments. Subendocardial-mid myocardial delayed enhancement of the mid-chamber anteroseptal wall and transmural delayed enhancement of the mid-chamber anterior wall raised suspicion for ischemic disease and non-viable myocardium, respectively.
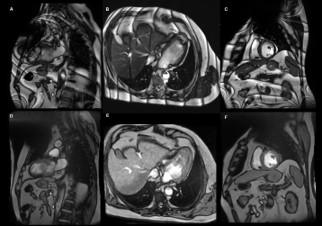
Figure 1: Cardiac magnetic resonance imaging cine images. (A-C) Steady-state free precession sequencing in the vertical long axis, horizontal long axis, and short-axis views, respectively, showing significant artifact, characterized by banding. (D-F) Fast gradient echo sequencing in the vertical long axis, horizontal long axis, and shortaxis views, respectively, with improved device-related artifact and moderately diminished myocardium-blood contrast.
The heightened impact of device-related artifacts on SSFP stems from its temporal resolution and robust signal-to-noise ratio, facilitating clear differentiation between the myocardium and blood. This is achieved through several factors: rapid repetition times (TR) between successive pulses; short echo time (TE), delineating the time between pulse delivery and signal acquisition; and a high flip angle, representing the net rotational dynamics during pulse application. While SSFP’s susceptibility to off-resonance artifacts and subsequent magnetic field inhomogeneity is primarily attributed to its short TE, it also facilitates high-speed imaging and improves tissue contrast, thus allowing for the assessment of both structural and dynamic (e.g., blood flow, cardiac motion) processes [4].
A lesser known alterative is the GRE sequence characterized by slow TR, long TE, and low flip angles which substantially lowers the risk of non-diagnostic imaging by nearly 96% [3]. Compared to SSFP, the longer duration of TE in GRE results in a significantly lower number of artifacts and improves image quality (odds ratio: 3.5; p<0.0001) [2], as well a greater sensitivity for detecting turbulent flow (e.g., valvular disease) [1,2,4].
The advantages of GRE over SSFP occur at the expense of tissue contrast and temporal resolution [1,2,4]. Myocardial-blood contrast is crucial for parametric mapping with cine imaging and quantitative assessment of myocardial function. Short-axis images are paramount in this context; however, they are disproportionately affected by artifacts, especially when SSFP is employed compared to GRE [1,2,4]. In this scenario, image quality issues, such as low contrast and blurring, may require manual refinement if automated mapping software is used, whereas nonanalyzable images might benefit from SSFP with the arm positioned above the head [2].
GRE has also demonstrated utility in contrast-enhanced perfusion imaging, which requires rapid image acquisitions to assess the risk of myocardial ischemia. Despite its lower temporal resolution, when compared to SSFP, GRE has shown impressive diagnostic efficacy in 98% [1] of cases undergoing perfusion imaging.
Recent years have witnessed significant technical advancements in cMRI, leading to the expansion of its indications. Not long ago, patients with an ICD were ineligible for cMRI; however, many are still denied this crucial diagnostic tool due to device-related artifacts. In such cases, GRE has emerged as a promising alternative to traditional cMRI sequences. Therefore, for patients with an ICD an initial attempt at cMRI using SSFP cine imaging may be conducted. If image quality is compromised, switching to GRE sequencing can enhance image quality and optimize patient care.
Disclosures: The authors declare that there is no conflict of interest.
Consent statement: Written informed consent was obtained from the patient.