Article Type: Case Report, Volume 2 Issue 1
*Corresponding author: Zhengang Wang
Beijing Tsinghua Changgung Hospital, No.168 Litang Road, Changping District, Beijing, China.
Email: 13641339910@163.com
Received: Jan 21, 2025 Accepted: Feb 18, 2025 Published: Feb 25, 2025
Citation: Yinghua Z, Ruohan Y, Zhengang W. Successful non-surgical treatment of laryngeal damage in a child patient with relapsing polychondritis and a literature review. Ann Case Rep Med Images. 2025; 2(1): 1015.
Copyright: Zhengang W et al. © All rights are reserved
Background: Relapsing Polychondritis (RP) is a rare autoimmune disease with children accounting for less than 5% of cases, and patients with tracheal chondritis have poor prognosis.
Case Presentation: Polyarthritis with fever was initially presented in a female patient of 12-year-old. Auricular chondritis, saddle nose and dyspnea developed within 3 months with airway imaging changes, leading to the diagnosis of RP, but poor respond to the combined treatment of steroids, csDMARDs and bioDMARDs. Consequently, a tracheostomy become inevitable. The patient was heavy restricted to speech and breath if the trachea cannula blocked artificially. With 3 times following up of 6 month-interval, a gradual improvement in extent of stenosis and block, even block-solved or re-open, was seen, with bioDMARDs discontinue and steroid tapering successful. And the patient was in good spirit of normal social activities in terms of verbal communication after backed to school since the first visit in our hospital.
Conclusion: It is suggestive that special attention should be paid to child patients with RP tend to laryngeal involvement. Strong and prolonged treatment with chronic disease management was necessary to avoid surgical intervention.
Keywords: Relapsing polychondritis; Tracheal chondritis; Tracheostomy; csDMARDs; bioDMARDs.
Relapsing Polychondritis (RP) is a rare autoimmune disease that mainly affects cartilage and tissues rich in proteoglycan components, manifesting as auricular chondritis, nasal chondritis, tracheal chondritis, arthritis, inflammatory eye diseases, and inner ear involvement. Auricular chondritis, arthritis, and tracheal chondritis are the top three common clinical manifestations of RP, with these symptoms occurring in 90%, 40-80% and 50% of patients respectively [1-4]. Patients with tracheal chondritis have poor prognosis, which is a common cause of death in RP. RP can occur at any age, with children accounting for less than 5% of cases, and the onset typically occurs within the range of 1.7 months to 17 years of age [5]. Due to the rarity and clinical diversity, there is a lack of widespread clinical validation for the criteria of diagnosis [6,7], evaluation [8] and treatment recommendations. It is described in this manuscript a process of successful non-surgical treatment in a pediatric patient with severe RP of laryngeal damage and tracheotomy, along with a literature review.
The 12-year-old female patient was firstly diagnosed with Juvenile Idiopathic Arthritis (JIA) due to the polyarthritis including right sternoclavicular joint and temporal-mandibular joint, with snoring and fever. High CRP (82 mg/L) and ESR (120 mm/h) was documented. The ANA in titer of 1:160 was showed with all other autoantibodies negative including ENA, anti-CCP antibody, RF, HLA-B27 and ANCA. Normal pulmonary CT scan was indicated, and thicker epiglottis was shown by cervical CT scan. Furthermore, the inflammatory signal was gathered by cervical MRI. Subsequently steroid, leflunomide, sulfasalazine and Tumor Necrosis Factor Inhibitors (TNFi) were used, which was proved ineffective. Three months later, pinna chondritis, alongside saddle nose and bilateral temporomandibular joint pain developed. A cervical CT repeated the substantial soft tissue thickening around the glottic and subglottic areas, leading to localized laryngeal airway lumen narrowing. Relapsing Polychondritis (RP) was diagnosed with higher inflammation state (CRP 219 mg/L and ESR 110 mm/h), and pulse steroids and Methotrexate (MTX) were used with TNFi. However, significant improvement was not observed soon. The symptoms due to airway blocking continued and deteriorate culminating in sudden dyspnea and followed by endotracheal intubation and tracheotomy necessitated due to the inability to extubate. Ten months later the marked chest pain and elevated inflammatory state recurred when steroid dosage reduced to 35 mg daily while MTX and TNFi maintaining. Worse condition of laryngeal airway narrowing, and local block was showed by the third cervical CT scan accompanied by thickened surrounding soft tissues. Consequently, the regimen was substituted by Cyclophosphamide (CTX) and Interleukin-6 Receptor Inhibitor (IL-6ri) besides steroids. After then, it remained stable with normal ESR and CRP for a period in the following 3 months. But the trachea cannula could not be blocked and extubated, which significantly impacting her daily life and was compelled to discontinue her education.
She was hospitalized in our facility on Feb 28 in 2023 because of unbearable pain in rib and the temporomandibular joint area after further steroids tapering another half year later, approximately a year and a half after disease onset. Cushing syndrome, saddle nose, joints tenderness without pinna chondritis and ocular abnormalities were documented, dyspnea appears soon within few minutes after trachea cannula blocked, and hoarse voice with anxiety was noticed upon admission. Substantial blocking of laryngeal airway by surrounding thickening soft tissues with cricoid cartilage diminished was reviewed by cervical CT scan (Figure 1a & 1e).
To alleviate her condition, a thorough assessment and judgment was done including a plan of management for medical education, homecare and follow-up. Azathioprine (AZA) was added to her current regimen. A notable and gradual resolution with cricoid cartilage calcification were observed in the serial cervical CT scan after each 6 months follow-up, with steroid tapering further (Figure 1b & 1f) and bioDMARDs tapering (Figure 1c & 1g). Moreover, with steroid in a small doge, her condition continued to improve after bioDMARDs discontinuing (Figure 1d & 1h). Especially, with our encourage, she had gone back to school with good spirit and successful social communication in terms of verbal speech, when trachea cannula could be blocked artificially without dyspnea for two hours.
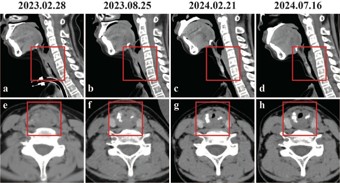
Figure 1: Dynamic image changes of laryngeal damage improving. (A,E) Laryngeal stenosis with blockage by marked soft tissue in inflammation and blurry margins of boxed area were seen upon admission. (B,F) Shrinkage of the area of laryngeal blockage and spots of calcification were seen in first follow-up six months after the treatment. (C,G) Further shrinkage to almost unobstructed were seen with calcified spot increased in the second follow-up twelve months after the treatment. (D,H) Even still narrowing, the laryngeal tract was unobstructed in the third follow-up seventeen months after the treatment.
The diagnosis of Relapsing Polychondritis (RP) mainly relies on clinical manifestations and differential diagnosis. This case presented initially with fever and widespread joint pain, which led misdiagnosis of Juvenile Idiopathic Arthritis (JIA). However, subsequent developments in the patient’s condition, including pinna chondritis, saddle nose and airways involvement, lead to a final diagnosis of RP, which fulfilled the criteria of Michet’s and Rose’s [6,7].
It is reported that, in adults, arthritis was the second most common symptom to pinna chondritis, whereas in children, arthritis is the most frequent symptom [1,2,5], which is nonerosive, lack of specificity, affecting joints in whole body with sternoclavicular joints typical involvement. Cases with polyarthritis as initial manifestation are prone to be misdiagnosis [9], as the case in this manuscript. The arthritis in temporomandibular joint can be seen in many inflammatory arthritis, but scarcely in RP, by which the clinical significance was discussed in reference [10].
The type of RP onset and progress is with significant heterogeneity. After the polyarthritis, three important regions of cartilage organ (ears, external nose, and airway) escalated rapidly within three months accompanied by high inflammatory state with severe laryngeal obstruction necessitated tracheostomy finally, meeting the criteria of acute progressive and severe type of RP [3]. Studies on airway involvement in RP in the past mostly focus on lower airway changes with research on laryngeal involvement limited. It is found that approximately 25% of patients develop laryngotracheal stenosis [11], and half of RP patients have hidden involvement of airways [12], and children’s patients with RP exhibit a worse prognosis when their airways are affected and tracheostomy due to laryngeal airway involvement is more common than adults [13]. Hence, clinicians should detect early signs of tracheal involvement.
The current case highlights premonitory signs of laryngeal involvement as followings. 1. Hoarseness: It is a common symptom in RP with laryngeal involvement, indicative of lesions affecting the vocal cords or surrounding structures [14]. In this case, hoarseness was documented with disease progression, but not in initial. 2. Snoring: Snoring occurs when breathing is partially obstructed by relaxed laryngeal tissues. It is shown in a study that frequent heavy snoring (four times or more at night per week) in children is indicative of non-benign conditions [15]. It is proved that the emergence of snoring in this case signified early signs of laryngeal involvement. 3. Imaging: By serial imaging of cervical CT scan of this case, it is reviewed a dynamic progress in laryngeal airway lesions, but lack of enough attention. On the other side, the process of imaging resolution is another strong evidence for confirmation of laryngeal involvement in patients with RP.
The treatment of RP is challenging. Existing recommendation predominantly adhere to a strategy of anti-inflammatory like the treatment of other rheumatic disease, with personalized scheme depend on organs involved and its influence on outcomes [16]. The therapeutic arsenal comprises of steroid being the first line, csDMARDs and bioDMARDS. However, it is lacking clinical verification. It is reported that overall response rate was 2/3 over a period of six months treatment with a complete response rate of just 19% [11]. Consequently, treatment regimens are frequently modified in a stepwise manner based on the observed therapeutic outcomes [17]. Unfortunately, inadequate response was observed in this patient despite combined treatment with potent steroids, csDMARDs and bioDMARDs.
There are many factors need to considerate for a new treatment in this patient. Firstly, multiple organs involved including airway and RPDAI score of 46 points which indicated the severity of disease [16]. Secondly, rapid progression with comprehensive respiratory involvement aligns with the severe subtype of RP [3], suggestive poor prognosis. Thirdly, relative shorter course of 18 months comparing with the average delay of 2.9 years [18] of diagnosis, indicating still in active stage (predominantly inflammation rather than fibrosis by pathology). Last, possible drug resistance of partial response to multiple drug treatments, but still in difficulty in steroid tapering. So, despite the great challenges in drug selecting, more aggressive treatment still retains valuable.
Medical adherence is important for improving outcomes in many chronic diseases (such as diabetes) [19], which was influenced by many factors such as patient’s education and recognition on common knowledge of the disease. Outlined fundamental aspects of management plan for patients with RP has been suggested [3] though lacking of empirical clinical research.
The patient in this manuscript is well cooperative while disease education and follow-up, and actively involved with positive attitude in daily life while schooling and homecare. The high level of compliance is one of the reasons crucial for ensuring the efficacy of treatment, in preventing infections, particularly in backing to society.
Currently, there is a scarcity of scholarly literature dedicated to RP in children. This study tracks the process of development, treatment and improving meticulously in a child patient with RP of airway involved in rapid progress style, presents radiological evidence for laryngeal involvement and the social results with chronic disease management of RP.
Ethics and patient consent: The written informed consent from the patient for the publication has been obtained.
Conflict of interest: The authors declare no competing interests.