Article Type: Case Report, Volume 1 Issue 1
*Corresponding author: Reem A Alqusaimi
Al Amiri Hospital, Kuwait City, Kuwait.
Email: reem.alqusaimi@hscm.ku.edu.kw
Received: Aug 21, 2024 Accepted: Oct 16, 2024 Published: Oct 23, 2024
Citation: Alqusaimi RA, Alzayed JA, Alawadhi AA. Pemphigus vegetans: A case report and review of literature. Ann Case Rep Med Images. 2024; 1(1): 1010.
Copyright: AlQusaimi RA et al. © All rights are reserved
Background: Pemphigus Vegetans (PVeg) is a rare variant of pemphigus vulgaris, an autoimmune blistering disorder typically affecting adults. It is characterized by hypertrophic vegetating lesions and flaccid pustules, often preceded by le- sions in the oral cavity.
Case presentation: We present the case of a 23-year- old male with a history of oral ulcers, a painful and pruritic genital rash, and extensive ruptured bullae and erosions on the trunk and back. A skin biopsy revealed focally acanthotic epidermis with prominent suprabasal clefts, intra epidermal vesicles, and neutrophilic micro abscesses. The dermis ex- hibited a dense perivascular and interstitial inflammatory infiltrate, predominantly composed of neutrophils and eo- sinophils. Direct immunofluorescence further supported the diagnosis of PVeg. The patient was treated with systemic corticosteroids and a single cycle of intravenous Rituximab, resulting in significant improvement of the skin lesions.
Conclusion: This case underscores the importance of con- sidering PVeg in the differential diagnosis of vesiculobullous diseases and highlights the need for further research into its pathogenesis and optimal management strategies.
Keywords: Pemphigus; Vesiculobullous; Autoimmune.
Pemphigus is an autoimmune vesiculobullous disorder characterized by autoantibodies targeting the surface antigens of keratinocytes or adhesion molecules. It is primarily categorized into two main forms: Pemphigus Vulgaris (PV) and pemphigus foliaceus. PVeg is a rarer variant of PV, clinically defined by hypertrophic vegetating lesions, flaccid pustules, or cauliflowerlike plaques. These lesions most often appear in flexural or intertriginous areas and the oral mucosa, although they can occur anywhere on the body. PVeg has two main subtypes: Hallopeau PVeg and Neumann PVeg. While both share similar clinical, immune pathological, and histological features, they differ in prognosis and disease progression. The Neumann subtype typically presents with periorificial papillomatous vegetations, whereas the Hallopeau subtype is marked by pustules that develop into vegetations, primarily affecting intertriginous areas [1]. PVeg accounts for only 1-2% of all pemphigus cases. Literature analysis indicates that it can occur across all age groups, including children, but predominantly affects middle-aged adults, with a median onset age of 40-50 years. The sex ratio is approximately 4.66 (14 females to 3 males), and there is usually no family history of bullous dermatosis [2]. In this report, we present the case of a 23-year-old Indian male who initially presented with a two-week history of oral ulcers, accompanied by a painful genital and penile rash that rapidly progressed to involve the rest of his body a week later. The diagnosis of PVeg was confirmed through histopathological and immunological evaluations. This case underscores the challenges associated with diagnosing and managing patients with PVeg.
A 23-year-old, previously healthy, Indian male presented to the emergency department complaining of a two-week history of oral ulcers associated with genital and penile rash. One week after the initial presentation, lesions on different areas of the body started to appear. These lesions were described to be painful, pruritic and associated with malodorous discharge. According to the patient, the rash was associated with constitutional symptoms, such as fever, sore throat, rhinorrhoea, generalized body aches and loss of appetite. Upon further history taking, the patient disclosed having sexual intercourse three months ago. There were no history of drug ingestion nor recent travel. In the emergency department, an initial diagnosis of Monkeypox was established, and hence the patient was shifted to isolation for further investigation. Thereafter, three swabs were taken; nasopharyngeal, vesicle and crusts, all of which did not detect Monkeypox virus. Keen examination of the face revealed eroded lesions between the eyebrows, surrounding the nostrils involving the nasal mucosa, as well as on the lips. The oral cavity was also affected, as ruptured bullae and erosions were also observed on the lateral aspect of the tongue (Figure 1). Characteristic erosions and ruptured bullae, followed by the formation of vegetative plaques, were also seen on the trunk and the genital area (Figure 2). The patient was vitally stable and afebrile. Routine blood work up, including complete blood count, renal and liver function tests and bio chemistry, were ordered. All of which appeared to be within the normal range, except for a mild leucocytosis, predominantly eosinophilic. To rule out infectious causes, an extensive screening panel, including syphilis, Epstein Barr virus, cytomegalovirus, Hep B virus and HIV, was conducted. All of which appeared to be negative. Histopathological evaluation of the skin biopsy revealed focally acanthotic epidermis with prominent suprabasal clefts, intra epidermal vesicles and neutron philic micro abscess formation. Therewas also marked acantholysis, resulting in the formation of ‘tombstone’ appearance of the lower epidermal cells. The dermis showed a dense perivascular and interstitial inflammatory infiltrate composed predominantly of neutrophils and eosinophils. Other cells, such as lymphocytes and histiocytes, were also present. The dermal papillae demonstrate edema and are infiltrated by neutrophils (Figure 3). Through direct immunofluorescence, intercellular deposits of IgG and C3 were observed on the surface of keratinocytes (Figure 4). Enzymelinked immunosorbent assays for both anti-desmoglein 3 and anti-desmoglein 1 antibodies revealed elevated titers. These results were most consistent with the clinical impression of PVeg. The treatment plan included the use of Prednisone at doses of 1 mg/kg every 24 hours until cessation of new lesion formation, followed by a tapering course. The patient was also given a single cycle of Rituximab, intravenously. There was a marked improvement in the skin lesions following the stated course of treatment (Figure 5).

Figure 1: Clinical findings of pemphigus vegetans; Labial and oral involvement.

Figure 2: Clinical findings of pemphigus vegetans; Involvement of trunk and genital area.
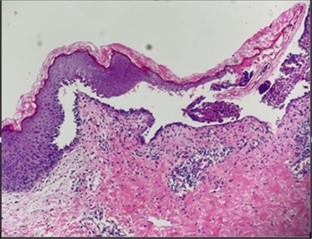
Figure 3: Histopathological examination of skin biopsy using haematoxylin and eosin stain.
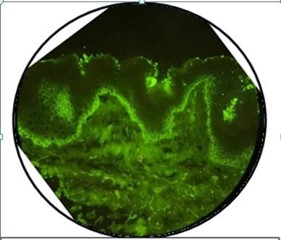
Figure 4: Direct immunofluorescence findings.

Figure 5: Follow-up results.
P Vegis a rare skin disorder that is speculated to represent a reactive pattern to autoimmune insults associated with PV. The skin lesions of PVeg vary and are characterized by vesicles and erosions that develop into hyperkeratotic vegetating masses. These lesions predominantly affect intertriginous areas, such as the axillary, inframammary, inguinocrural, and intergluteal regions, and invariably involve the oral mucosa. Oral lesions, often appearing as cerebriform-shaped formations, are seen in nearly all PVeg cases and can sometimes lead to malnutrition. Other areas with small folds, including the nasolabial and labial folds and the periumbilical region, may also be affected. Initially, lesions in PVeg are confined to a single site, usually the oral mucosa, but can become multifocal over time, with varying involvement of body surface area [3]. The literature describes two main subtypes: Neumann PVeg and HallopeauPVeg. The Neumann subtype typically has a prolonged and unremitting course, showing more resistance to treatment. Lesions associated with this type include vesicles and bullae that form vegetating masses with pustules, alongside oral erosions. Rare cases of verrucous masses confined to the oral cavity have also been reported, which can rapidly spread to the lips and become intensely pruritic. Conversely, the Hallopeau subtype is milder, characterized by pustules that evolve into vegetating plaques and is associated with spontaneous remission, unlike the Neumann type [4]. Due to its rarity, the aetiopathogenesis of PVeg remains unclear. The development of vegetating lesions in intertriginous areas may be attributed to relative occlusion and maceration, potentially leading to secondary bacterial infection. There is also a genetic component to pemphigus, with a significant association with class II HLA antigens. All variants are marked by the production of pathogenic autoantibodies targeting different desmosomal proteins. In PVeg, antibodies primarily react with the same antigens as in PV, specifically desmoglein 3 and, to a lesser extent, desmoglein 1. Antibodies against desmoglein 3 lead to suprabasal acantholysis, while those against desmoglein 1 cause subcorneal acantholysis in the epidermis. Studies have indicated that PVeg may also be linked to antibodies targeting other desmosomal proteins, such as desmocollins 1 and 2, and periplakin. Additionally, immunopathological factors, including Th2-mediated immune reactions (such as interleukin-4), along with IgG autoantibodies and cytokines, play a role in the epithelial proliferation and eosinophil chemotaxis observed in P Veg [3]. Contributing factors to the development of P Veg include HIV infection, intranasal heroin use, captopril treatment, and organ transplantation [2]. Diagnosis of P Veg primarily relies on clinical manifestations, cyto diagnostic examinations, such as the Tzanck test, and histopathology. The Tzanck test reveals acantholytic cells along with characteristic cytological phenomena, including Sertoli’s rosettes and leukocyte adherence forming streptocytes. An accurate diagnosis is confirmed through skin biopsy, where PVeg lesions typically show indistinct suprabasal acantholysis, irregular epidermal hyperplasia, papillomatosis, and microabscesses containing eosinophils and neutrophils, sometimes interspersed with apoptotic or necrotic keratinocytes. The dermis often appears edematous, with elongated papillae forming protruding villi, vasodilation, and intense mixed inflammatory infiltrates. Immune fluorescence findings in PVeg are indistinguishable from those in PV, with direct immunofluorescence showing deposition of IgG and C3 on keratinocyte surfaces and indirect immunofluorescence revealing circulating anti-epithelial cell-surface IgG [3]. Given the characteristic lesions in PVeg, differential diagnoses are limited. In cases with oral lesions, potential differentials include pyosto matitisvegetans, aphthous ulcers, or erosive lichen planus. Vegetating lesions in intertriginous regions must be differentiated from chronic infections, such as condylomata acuminata, condylomatalata, candidal intertrigo, blastomycosis, or Hailey-Hailey disease. Lesions affecting non-intertriginous regions should be differentiated from seborrheic keratoses [5]. Treatment for PVeg is similar to that of PV, with systemic corticosteroids being the initial treatment of choice. Adding immunosuppressive agents can improve remission rates and promote a steroid-sparing effect. These agents include azathioprine, dapsone, cyclophosphamide, mycophenolate mofetil, and cyclosporine. For localized forms of PVeg, topical or periodic intralesional corticosteroids are recommended and can lead to quick recovery, even with significant lesions. In cases of recalcitrant vegetating lesions, alternative regimens, such as a combination of nicotinamide with tetracycline and etretinate, or corticosteroids with etretinate, may be considered. For resistant cases, extracorporeal photopheresis, pure silver nitrate application, carbon dioxide laser treatment, or even surgical excision have been proposed, and TNFα inhibitors have been used in therapyrefractory patients [5]. Prognosis in PVeg has been analyzed in a limited number of studies, indicating that younger age at diagnosis is associated with a worse course and outcome. Other factors predicting poor outcomes include mucosal involvement and inadequate response to treatment. Various complications have been reported, primarily related to prolonged systemic corticosteroid therapy [5].
Given its rarity and diverse clinical presentation, pemphigus vegetans (PVeg) can pose challenges for initial diagnosis and subsequent treatment. This case emphasizes the importance of including PVeg in the differential diagnosis of vesiculobullous diseases and highlights the need for further research to clarify its pathogenesis, improve diagnostic accuracy, and establish optimal management strategies.
Statement of ethics: Informed consent was obtained from the patient for publication of this case and accompanying images.