Article Type: Short Report, Volume 1 Issue 1
*Corresponding author: Sebastian Słomka
Department of Internal Medicine and Geriatrics, Bieganski Hospital, Lodz, Poland.
Email: sslomka@wp.pl
Received: Aug 02, 2024 Accepted: Sep 04, 2024 Published: Sep 11, 2024
Citation: Zięba P, Słomka S. Stroke as the first sign of heart tumor- What the neurologist should know about heart. Ann Case Rep Med Images. 2024; 1(1): 1005.
Copyright: Słomka S et al. © All rights are reserved
Primary heart cancers are rare, but cancer metastases occur much more often, which is why they are diagnosed mainly in non-oncology departments. Approximately 85% of heart cancers are benign, with myxoma predominating [1,4].
A 37-year-old female patient referred for a routine cardiology consultation by a neurologist diagnosing the causes of stroke. The patient was hospitalized in the neurological ward due to numbness of the left half of the body, dizziness with vomiting, transient speech disorders, drooping eyelid of the left eye. A CT scan of the brain was performed, followed by an MRI, where 3 hyperintense foci described as vascular or inflammatory were imaged.
A cardiology consultation took place about 3 months later, during the examination the doctor found a diastolic murmur (about 3-4/6 according to Levin) the loudest above the apex, non-radiating, variable in respiratory terms (it was reduced on inspiration) and split heart tone. ECG sinus rhythm 73/min, normogram, rSr’ in V1-2; PQ-134 ms.; QTc-412 ms. TTE showed a large, mobile tumor measuring 54 x 26 mm with numerous projections extending onto the peduncles from the septal wall of the left atrium. During movement, the formation partially moved into the lumen of the left ventricle, causing an increased transvalvular gradient (V max. 1.8 m/s, gradient max 13 mmHg, gradient mean 2.8 mmHg), moderate mitral regurgitation (II*) and enlargement of the left atrial cavity (41 mm in LAX).

Figure 1: Left atrium tumor with LAX diastole.
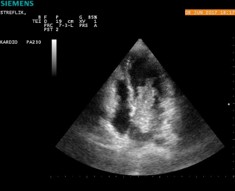
Figure 2: Tumor within the left atrium in diastole in the four-cavity apical projection.

Figure 3: Tumor within the left atrium in diastole in the four-cavity apical projection.

Figure 4: Tumor mass dimensions in LAX projection.

Figure 5: Intraoperative photograph showing left atrial tumor (black arrow).

Figure 6: Resected tumor.

Figure 7: Postoperative condition - after removal of the tumor in the LAX projection.
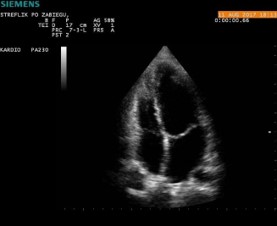
Figure 8: Condition after surgery - after removal of the tumor in the four-cavity apical projection.
The patient was urgently referred to a cardiac surgery unit, where the tumor was removed. Histopathological examination described myxoma. In the follow-up TTE study, 2 months after the procedure, a decrease in the size of the left atrial cavity (34 mm. in LAX) and moderate mitral regurgitation (II*) were observed, the other parameters were within the norms. Six months after the procedure in control TTE was smaller mitral regurgitation (I*), the patient did not feel any symptoms and returned to amateur sports in full range.
The described case is an example of one of the four basic clinical masks of left atrial myxoma, which include: heart failure, arrhythmias and conduction disorders, embolic events, as well as mechanical damage including mitral regurgitation and mitral ostium stenosis, which may be manifested by syncope [1-3]. Myxoma is the most common primary cancer of the heart [4,5]. It is more common amongst women (about 70%) in the 3rd-6th decade of life [5]. It can reach considerable sizes (up to 15 cm) and a weight of up to 180 grams. It may have numerous protrusions, which promotes the formation of] thrombi and, as a result, embolic complications. Symptoms depend on the location of the lesion. It most often arises in the left atrium in the area of the fossa ovale, causing embolism in the systemic circulation and peripheral ischemia of the limbs, while its location in the right part of the heart promotes pulmonary embolism [3]. It is estimated that peripheral embolisms occur in about 40-50% of patients [6]. Transthoracic Echocardiogram (TTE) is the test of choice, and in cases of atypical location, multifocal lesion or non-pedunculated myxoma, it is necessary to use Transesophageal Echocardiography (TEE), computed tomography or magnetic resonance imaging of the heart [7]. The last two studies provide additional information about the type of tissue from which the tumor is built and about the infiltration of surrounding structures, including vessels. Early diagnosis of primary heart cancer is often critical to a patient’s prognosis. The only method of treatment is surgical excision of the tumor. Usually, severe complications and deaths of patients occur while waiting for surgical treatment [8], which justifies the rush to refer every patient with a cardiac tumor to the cardiac surgery department. It should be remembered that patients, despite the fact that they are cured, should still be monitored due to the risk of recurrence and the possibility of malignancy, which is why they are treated as locally malignant neoplasms. In the above-discussed clinical case, the neurologist’s decision to urgently consult a cardiologist and perform an echocardiographic examination (TTE), and consequently to perform an urgent procedure, contributed to the patient’s avoidance of disability and possibly death. In conclusion, it should be emphasized that echocardiography in patients with symptoms of systemic embolism, including cerebral embolism, is justified and should be recommended in any case.