Article Type: Short Report, Volume 1 Issue 1
*Corresponding author: Arnabjyoti De
Mahatma Gandhi Medical College and Research Institute, Puducherry, India.
Email: arnabjyotide74905@gmail.com
Received: Jul 22, 2024 Accepted: Aug 13, 2024 Published: Aug 20, 2024
Citation: Arnabjyoti De. Development of rhinitis medicamentosa in young chronic nasal drop users. Ann Case Rep Med Images. 2024; 1(1): 1003.
Copyright: Arnabjyoti De et al. © All rights are reserved
Rhinitis Medicamentosa (RM), commonly known as rebound nasal congestion, is an increasingly prevalent condition among young individuals who chronically use topical nasal decongestants. This article explores the development of RM, highlighting the mechanisms, clinical features, prevalence, risk factors, and management strategies. RM arises from the prolonged use of nasal decongestants, leading to receptor down-regulation, rebound vasodilation, and inflammatory changes in the nasal mucosa. Clinically, RM is characterized by persistent nasal congestion that does not improve with continued decongestant use. The risk factors include chronic rhinitis, lack of awareness about proper medication use, and the easy accessibility of over-the-counter decongestants. Prevention of RM focuses on patient education and adherence to recommended usage guidelines, while management involves discontinuing decongestants and employing alternative therapies such as saline sprays and nasal corticosteroids. This article underscores the importance of awareness and proper education to prevent RM and highlights effective management strategies for those affected.
Keywords: ORhinitis; Nasal drops; Nasal decongestants; Oxymetazoline.
Rhinitis Medicamentosa (RM), often referred to as “rebound nasal congestion,” is a condition triggered by the overuse of topical nasal decongestants. This phenomenon, characterized by persistent nasal congestion without an underlying allergic or infectious cause, is becoming increasingly prevalent among young individuals who use nasal drops chronically. This article explores the development of RM in young chronic nasal drop users, its underlying mechanisms, clinical features, and strategies for prevention and management.
Mechanisms and pathophysiology
Topical nasal decongestants, such as oxymetazoline and phenylephrine, are commonly used to relieve nasal congestion by constricting blood vessels in the nasal mucosa. However, with prolonged use (typically beyond three to seven days), these medications can lead to a paradoxical increase in nasal congestion. The exact mechanisms underlying RM involve several factors:
Receptor down-regulation: Chronic use of decongestants leads to the down-regulation of alpha-adrenergic receptors, reducing the responsiveness of nasal blood vessels to the constricting effects of the medication [1].
Rebound vasodilation: Upon withdrawal of the decongestant, a rebound vasodilation occurs, exacerbating nasal congestion [2].
Inflammatory changes: Chronic use induces inflammatory changes in the nasal mucosa, including epithelial cell damage and increased vascular permeability [3].
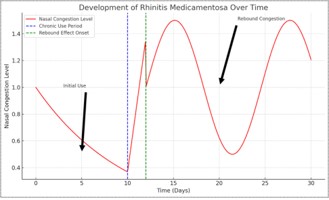
Figure 1: Illustrates the development of rhinitis medicamentosa over time. The x-axis represents time in days, while the y-axis shows the level of nasal congestion.
Initial use (days 0-10):The nasal congestion decreases initially due to the effective use of nasal decongestants.
Chronic use period (around day 10):Continued use leads to a stabilization of congestion levels, representing the period of chronic use.
Rebound effect onset (after day 12):Once the use of nasal decongestants stops, rebound congestion sets in, causing a significant increase in nasal congestion.
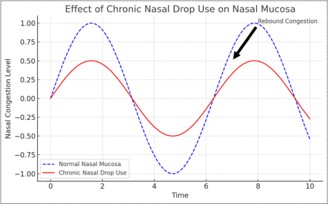
Figure 2: Shows the effects of chronic nasal drop use on nasal mucosa. The blue dashed line represents normal nasal mucosa with typical variations in congestion, while the red line shows the increased congestion due to chronic nasal drop use, highlighting the rebound congestion effect. This clear visual underscores how prolonged use of nasal decongestants can lead to worsened nasal congestion over time.
Clinical features and diagnosis
RM presents primarily with persistent nasal congestion that does not improve with continued use of nasal decongestants. Patients often report a history of prolonged use of these medications beyond the recommended duration. Physical examination may reveal swollen, erythematous nasal mucosa without significant discharge. Diagnosis is largely clinical, based on history and presentation, but it can be supported by rhinoscopy findings [4].
Prevalence and risk factors
The increasing availability and over-the-counter status of nasal decongestants contribute to their widespread use and potential misuse, particularly among younger populations. Factors that increase the risk of developing RM include:
Chronic rhinitis: Individuals with chronic allergic or nonallergic rhinitis are more likely to use nasal decongestants frequently.
Lack of awareness: Many young users are unaware of the potential for developing RM and the recommended duration of use.
Accessibility: The ease of obtaining nasal decongestants without a prescription facilitates their overuse [5]
Prevention and management
Preventing RM involves educating patients about the risks associated with the prolonged use of nasal decongestants and promoting adherence to recommended guidelines. For those already affected, the management strategies include:
Discontinuation of decongestants: Gradual weaning off the medication or abrupt cessation, although the latter can initially worsen symptoms.
Alternative therapies: Use of saline nasal sprays, nasal corticosteroids, and oral decongestants can help alleviate symptoms during withdrawal.
Patient education: Informing patients about the proper use of nasal decongestants and encouraging regular follow-up to monitor adherence and symptom improvement [6].
Rhinitis medicamentosa is a preventable condition that significantly impacts quality of life, particularly in young individuals who chronically use nasal drops. Awareness, proper education, and adherence to usage guidelines are crucial in preventing RM. Healthcare providers should emphasize these aspects during patient interactions to reduce the incidence of this condition and promote effective management strategies for those affected.
Funding: This article received no external funding.
Competing interests: The author declares no competing interests.
Ethical approval: This article does not contain any studies with human participants performed by the author.