Article Type: Case Report, Volume 1 Issue 1
*Corresponding author: Maria Natale
Specialization School in Pediatrics, University of Bari “Aldo Moro”, Bari, Italy.
Email: m.natale10@studenti.uniba.it
Received: Jul 18, 2024 Accepted: Aug 09, 2024 Published: Aug 16, 2024
Citation: Muggeo P, Natale M, Maggi N, Grassi M, Raguseo C, et al. Ecthyma-like lesion in a boy with chronic disseminated candidiasis and acute lymphoblastic leukemia: An iceberg beyond the tip. Case report and literature review. Ann Case Rep Med Images. 2024; 1(1): 1002.
Copyright: Natale M et al. © All rights are reserved
Background: Chronic disseminated candidiasis is a clinical condition severely affecting patients with hematological malignancies. It has been mainly reported in adult patients, while cases in children and adolescents are rare. Diagnosis is challenging and not well established yet, but a thorough clinical examination can be helpful.
Case presentation: We present the case of a 15-year-old boy with B-cell precursor acute lymphoblastic leukemia who developed febrile neutropenia during induction chemotherapy. A cutaneous ecthyma-like lesion allowed to make the diagnosis, leading to the prompt initiation of therapy with liposomal amphotericin B and caspofungin. However, despite targeted antifungal treatment, the persistence of fever, evidence of neutrophil recovery and increased inflammatory markers raised suspicion of Inflammatory Immune Reconstitution Syndrome. Therefore, we added adjuvant therapy with glucocorticoids allowed to achieve clinical recovery.
Conclusion: Although rare, the occurrence of chronic disseminated candidiasis should be considered in pediatric and adolescent patients. In our patient, a single ecthyma-like lesion was the key to the diagnosis. Adolescents undergoing treatment for acute lymphoblastic leukemia face an increased risk of infectious complications and worse outcomes. We also highlight the importance to continue chemotherapy alongside antifungal therapy to achieve remission of both leukemia and fungal infection.
Keywords: Chronic disseminated candidiasis; Acute lymphoblastic leukemia; Ecthyma-like lesion; Candida tropicalis; Glucocorticoids.
Chronic Disseminated Candidiasis (CDC), also known as hepatosplenic candidiasis, is a rare and unique form of invasive disease caused by Candida spp, likely due to an imbalanced immune response that leaves to a major inflammatory reaction resulting in an immune reconstitution inflammatory syndrome [1-3]. It mainly affects organs such as the liver and spleen and may occur in patients with hematological malignancies, particularly during prolonged periods of neutropenia [4].
CDC represents a challenging condition that affects the morbidity and mortality in hemato-oncological patients [5], both due to the infectious disease itself and the delay in anticancer treatment. The treatment with antifungal drugs is considered the first choice, however the use of adjuvant corticosteroids represents the turning point to achieve clinical recovery [6].
While the condition is more commonly reported in adults, there have been few cases in children and adolescents [7,8].
Here, we present the case of a 15-year-old boy affected by Bcell precursor acute lymphoblastic leukemia (BCP-ALL). A single cutaneous ecthyma-like lesion was crucial for the diagnosis of unexpected CDC. The patient displayed persistent fever despite the treatment with a wide range of antifungal drugs. The use of adjuvant glucocorticoid therapy played a key role in the patient’s recovery.
A 15-year-old boy was diagnosed with B-lineage acute lymphoblastic leukemia and started the chemotherapy treatment following the AIEOP-BFM ALL 2017 protocol. The bone marrow aspirate on day +15 of the treatment showed morphological and cytofluorimetric remission of leukemia, defining non-high risk (non-HR) disease, confirmed at the subsequent molecular analysis (day+33). On day +60 of chemotherapy he developed febrile neutropenia, (neutrophils 220/mmc; zenith temperature 40°C). The patient was then admitted to the hospital and treated with broad-spectrum antibiotics (cefepime) (Day 1). Blood culture (Day 2) revealed the presence of the Enterobacter cloacae complex.
On Day 3, despite no changes in his clinical condition, a rise of inflammatory markers was measured (C-reactive protein CRP: 24.6 mg/l and procalcitonin PCT: 26.2 ng/ml). On Day 4 the fever subsided. On Day 10, teicoplanin was added to the antibiotic treatment because of the growth of Staphylococcus aureus spp. in a throat swab from a patient with severe neutropenia. In the following days his temperature spiked along with odynophagia (Day 14). To this purpose, a neck and abdomen ultrasound, echocardiogram, and chest X-ray were performed, showing no abnormalities. On day 15 procalcitonin was negative, CRP was 50.5 mg/l and neutropenia persisted (neutrophils 370/mmc).
The boy remained febrile, prompting us to add antifungal and antiviral treatment (fluconazole and acyclovir) according to international guidelines [9]. Cefepime was replaced with piperacillin-tazobactam.
Nevertheless, CRP further increased (87 mg/l). Hence, a neck-chest-abdomen computed tomography (CT) scan and a bone marrow aspirate were performed. The CT scan was uneventful and the aspirate confirmed the remission of leukemia (Day 16).
On Day 18 the blood culture came back negative but the fever persisted. The central venous catheter (CVC) was suspected to be the cause of the bloodstream infection, so the CVC was removed and teicoplanin was replaced with daptomycin. The antifungal therapy was empirically changed to liposomal amphotericin-B (L-AmB). The microbiological culture of the central venous catheter tip did not grow any pathological microorganism.
Throughout this time the patient remained neutropenic.
On day 25, a lesion characterized by a central black area and red edges appeared on the right inner ankle. The lesion did not result painful when pressed (Figure 1). A swab taken from the skin after gently scratching the area, detected Candida Tropicalis spp. (Figure 2).
The lesion evolved into a sore similar to ecthyma. It appeared as a shallow ulcer covered by a crust, with the area around it turning purplish-red (Day 29) (Figure 3).
At the same time, firm and painless swelling occurred on the right side of the neck providing an explanation to the consistent odynophagia (Day 26) (Figure 4). An increase in neutrophil count was recorded (neutrophils 2070/mmc). To rule out invasive candidiasis, a neck-chest-abdomen CT scan was repeated, and it revealed multiple low-density lesions in the liver, spleen, kidneys, and lungs (Figure 5). Specifically, the neck area showed a deep right laterocervical hyperdensal lymph-node with colliquated nucleus and a maximum diameter of 17 mm (Day 28).
A “proven” invasive fungal infection was diagnosed, and caspofungin was added to the liposomal amphotericin-B therapy (L-Amb). For further investigation, an ultrasound-guided liver biopsy was performed (Day 30). The histology showed a mixture cytic, and granulocytic inflammatory elements, with necrosis of the hepatic cells but no evidence of cancer or fungal infection. No pathogens were detected from the liver biopsy. An infectious disease specialist was consulted and the treatment with piperacillin-tazobactam was stopped while L-Amb was continued. However, the patient still complained malaise and marked fatigue.
In the following days, the neutrophil count recovered (2090/ mmc), the blood cultures remained negative, but the fever persisted as well as the increased CRP (50.9 mg/l). Therefore, the suspicion of candidiasis-related immune reconstitution inflammatory syndrome (IRIS) was raised. Empirically, corticosteroids (hydrocortisone 6 mg/kg/day) were added (Day 36). The patient remained apyretic from that point onwards. Chemotherapy was resumed on Day 38. A diagnosis of chronic disseminated candidiasis was made, and the patient was discharged with a continuation of steroid therapy (prednisone 1.5 mg/kg/ day for 3 days, then slowly tapered over 54 days) and a switch to oral fluconazole (6 mg/kg/die). Caspofungin was discontinued on the day of discharge (Day 46) (Table 1). Chemotherapy continued until the end of the induction phase followed by a phase of high-dose methotrexate, a reinduction phase, and a randomizely assigned immunotherapy phase (before maintenance phase) with blinatumomab according to the AIEOP-BFM ALL 2017 ongoing protocol. The patient is currently on maintenance treatment and continued to take oral fluconazole for a total of 6 months. A total body CT scan performed after 3 months showed significant improvement in the liver, kidney and lung lesions, and a follow-up scan at 6 months revealed no evidence of infiltrative nodules. Throughout the course of treatment, the patient did not experience any further adverse effects.

Figure 1: Echtyma- like lesion with a central black area and red edges, not painful when pressed (Day 25).

Figure 2: Scarified echtyma- like lesion (Day 25).

Figure 3: Echtyma like lesion as a shallow ulcer covered by a crust, with the area around it turning purplish-red (Day 29).

Figure 4: Swelling of the neck (Day 26).

Figure 5: CT scan demonstrating hepatic, splenic and kidney hypodense lesions (Day 28).
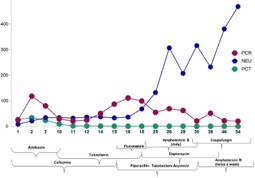
Graph 1: Trend of neutrophils and inflammatory markers. Medication’s scheme.
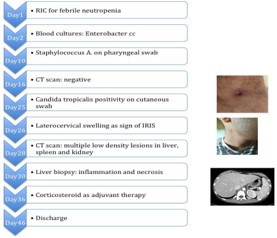
Table 1: Patient timeline.
CDC (Chronic Disseminated Candidiasis) is a rare infectious complication in patients with blood-related cancers undergoing aggressive chemotherapy. Furthermore, its rate of onset appears to be even more unusual in pediatric and adolescent patients compared to adults [7,8]. It is therefore crucial to be aware of this entity to early recognition and prompt treatment.
The pathophysiology is not well known, but it seems to start with Candida spp. colonization in the gastrointestinal tract, followed by invasion into the liver through the portal venous circulation [1,5].
After the fungus spreads during the neutropenic phase, a “paradoxical clinical deterioration” occurs when the neutrophil count rises within the optimal range. This stage is characterized by fever and the appearance of small nodules in the liver or spleen due to a pro-inflammatory immune response involving the recruitment of T-helper 1 (Th1) and T-helper 17 (Th17) cells, which in turn lead to the release of citokines such as tumor necrosis factor (TNF-α) and interferon-gamma. This immunological dysregulation promotes the immune reconstitution inflammatory syndrome [6].
The immune reconstitution inflammatory syndrome (IRIS) refers to the development of inflammatory disorders and an exacerbation of the symptoms in patients being treated for opportunistic infections, which cannot be explained by reinfection [10]. Thus, the use of corticosteroids appears to be the elective treatment for arresting the pro-inflammatory cytokine storm and restore a tolerogenic environment.
According to De Pawn et al. [11] the diagnostic criteria for proven yeast invasive fungal disease (IFD), revised for invasive fungal disease in children [12], require the growth of Candida spp. from blood or a sterile site. In this patient the swab taken from a sterile site after gentle scarification of the skin, allowed the demonstration of Candida spp. CDC is often the result of a previously misdiagnosed bloodstream infection from Candida spp [13] and symptoms usually do not occur until immune reconstitution [12].
The patient’s skin lesion at the site of the cultural sample is indicative of a specific disease, although not typical for a Candida species lesion. Candida Tropicalis has been rarely reported as the causative agent of acute invasive candidiasis in cases with skin lesions [14]. A recent case series of children with CDC also reported Candida Tropicalis in 4 out of 6 patients, with 3 of them having skin lesions [15]. However, skin lesions from C. tropicalis, whenever occur, are described as red maculopapular lesions [14], whereas the evolution into an ecthyma-like lesion as seen in our patient is not common.
Despite being a single lesion, the occurrence of an unusual skin lesion prompted us to conduct a microbiological examination and to repeat a total body computed tomography.
Early recognition of CDC is crucial to avoid life-threatening complications and delay in treatment, deleterious, especially in patients with pre-existing hematological malignancies.
The outcome depends on timely antifungal therapy, the severity of co-morbidity and the duration of treatment. The delay in the beginning of treatment for each 12-24 h may increase the mortality rate by up to 100% [16].
The treatment of CDC can be challenging, given the difficulty to detect fungi in cultures and considering that clinical responses usually take several weeks to become apparent. In addition, treatment approaches for CDC are mainly reported with a focus on adult patients [1,17,18].
Generally, the use of L-AmB is recommended as it is considered more effective until stable clinical conditions are achieved [19]. Echinocandins, particularly caspofungin, represent the newest class of antifungals with a fungicidal effect on Candida species. Step-down therapy, involving a transition from L-AmB or echinocandins to oral fluconazole administration, has shown favorable results [20].
In our patient, after 2 weeks of L-AMB treatment, the fever continued, so we added caspofungin. However, there was no apparent improvement in symptoms. Eight days later, we observed a significant change in the clinical scenario by empirically adding hydrocortisone. This confirmed that the fever was due to IRIS. According to the literature, fever may persist for weeks despite appropriate antifungal treatment, likely due to an immune reconstitution after neutrophil recovery [6]. Glucocorticoids play an essential role at this stage. We decided to administer hydrocortisone as adjuvant therapy, followed by prednisone.
A retrospective study involving 10 patients (6 adults and 4 children) with chronic disseminated candidiasis and persistent symptoms despite appropriate antifungal therapy demonstrated that prednisone treatment (0.5 mg/kg/day for at least three weeks) led to the resolution of fever and abdominal pain shortly after its administration (median four to five days) [6].
In CDC, the duration of treatment typically varies from several weeks to 6-12 months and it is adjusted individually [21]. In our patient, fever disappeared from the day of starting corticosteroid adjuvant therapy, which continued with slow tapering. The antifungal treatment was continued for a total 6 months.
Beyond early suspicion to prevent the clinical deterioration of patients, the CDC requires attention to avoid critical delays in anticancer treatment. While rare, this possibility should also be considered for pediatric and adolescent patients. In particular, adolescent patients undergoing treatment for acute lymphoblastic leukemia are at a higher risk of infectious complications and worse outcomes [22]. In our clinical case the detection of an ecthyma-like lesion was crucial to diagnose CDC, as it turned out to be an iceberg to deal with, beyond the tip.
CDC diagnosis is usually challenging due to the absence of specific markers; nevertheless, it is crucial to continue chemotherapy alongside antifungal therapy to achieve remission of both leukemia and fungal infection.
Acknowledgements: Not applicable.
Funding: No funding was received to assist with the preparation with the preparation of this manuscript. The authors have no relevant financial or non-finantial interests to disclose.
Employment: Not applicable.
Financial interests: None.
Non-financial interests: None.
Ethics approval: All procedures performed were in accordance with 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from parents. Ethical approval was waived by the local Ethics Committee in view of the retrospective nature of the report and because all the procedures being performed were part of the treatment protocol and supportive care, for which Ethical Approval has been previously obtained by the local Ethics Committee and already filed.
Consent: Informed consent was obtained from the parents.
Data and material: Clinical data and charts are available on request (Contact: Maria Natale email: m.natale10@studenti. uniba.it).